This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She is healthy with no known cardiac disease. A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. The morning before the cardiacarrest potassium was 4,3.mmol,
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5. Pacemaker mediated tachycardia!
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiacarrest, defibrillated, diffuse ST depression and ST Elevation in aVR.
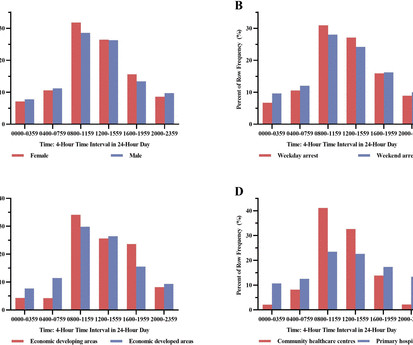
Background The circadian variation pattern of sudden cardiacarrest (SCA) occurred in Chinese community including both community healthcare centres and primary hospitals remains unknown. This study analysed the circadian variation of SCA in the Chinese community.
The 12-lead ECG and long lead II rhythm strip shown in Figure-1 — was obtained from a previously healthy, elderly woman who collapsed in the hospital parking lot. A series of cardiac arrhythmias were seen during the course of her resuscitation — including the interesting arrhythmia shown in the long lead II of Figure-1.
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Should you activate the cath lab?
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chest pain and SOB. The patient went into arrest pre-hospital. Junctional tachycardia? ).
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. AI recognizing cardiacarrests in emergency calls. Recently, hospitals have failed to identify 25% of cases of cardiacarrest.
MY Thoughts on ECG #1: The rhythm is sinus tachycardia at 105-110/minute. LEARNING Point: Maximal ST depression in leads V2-thru-V4 ( especially when the ST-T waves are shaped as they are in ECG #1 ) in a patient with new chest pain ( or sudden cardiacarrest, as in today’s case ) — is diagnostic of acute Posterior OMI until proven otherwise!
Is it ventricular tachycardia (VT) due to hyperK or is it a supraventricular rhythm with hyperK? Hospital admission had been recommended, but she left that ED against medical advice. If cardiacarrest from hypokalemia is imminent (i.e., A prehospital ECG was recorded: Limb leads: Precordial Leads What is the therapy?
There was 100% proximal LAD occlusion with TIMI 0 flow, and cardiacarrest in the cath lab. The patient had a protracted hospitalization and did not survive. There is sinus tachycardia at ~100/minute. In today's case — the sinus tachycardia may have been a harbinger of this patient's ultimate demise. As per Dr.
Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography. However, STE-aVR with multilead ST depression was associated with 31% in-hospital mortality compared with only 6.2% A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ).
Category 2 : An increase in myocardial oxygen demand due to tachycardia, elevated ventricular afterload (BP or aortic stenosis), or increased wall stretch (admittedly this latter is more complicated) or a decrease in oxygen supply due to hypotension, anemia, hypoxia, or a combination of all of the above. This results in Type I MI.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
3 studied 416 patients hospitalized with COVID in China, of whom 82 had an initial cTn(I) above the upper reference limit. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. Cardiac troponin I in patients with coronavirus disease 2019 (COVID-19): Evidence from a meta-analysis.
He had multiple cardiacarrests with ROSC regained each time. He spent almost 2 months in the hospital, and reportedly made a full neurologic recovery. This patient arrested shortly after hospital arrival. Hypercoagulability workup was positive for lupus anticoagulant. He was prescribed apixaban.
Written by Pendell Meyers We received a call from an outside hospital asking to transfer a "traumatic post arrest" patient. We received 4 ECGs, including his baseline on file, and three from today, including triage, peri-arrest, and post-ROSC (sorry for the poor quality due to scanning).
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Is it STEMI?
See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 Could the dysrhythmias have been prevented? mEq/L, from 1.9
BackgroundInhospital cardiacarrest (IHCA) is associated with significant morbidity and mortality. had ventricular tachycardia/ventricular fibrillation and 73.4% Journal of the American Heart Association, Volume 14, Issue 4 , February 18, 2025. Among 207 770 patients with IHCA, 26.6% had pulseless electrical activity/asystole.
This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent! Complete LMCA occlusion is associated with clinical shock and/or cardiacarrest. He was later transferred back to his local hospital neurologically intact and without serious sequela.
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
The patient was extubated on Day-3 of the hospital stay. The stay in the cardiac intensive care unit (CICU) was further complicated by sepsis, delirium, GI bleeding, and anuric renal failure with need for renal replacement therapy. However, he suddenly developed a series of malignant ventricular arrhythmias.
There is sinus tachycardia (do not be fooled into thinking this is VT or another wide complex tachycardia!) Plus recommendations from a 5-member panel on cardiacarrest. in-hospital mortality was 18.8% She was alert and oriented and hypotensive with initial BP 70/50. for AMI with new RBBB alone).
After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. Steve, what do you think of this ECG in this CardiacArrest Patient?" A woman in her 50s with dyspnea and bradycardia A patient with cardiacarrest, ROSC, and right bundle branch block (RBBB).
Other than tachycardia, Other than slight tachycardia, vitals were within normal limits (including oxygen saturation). About two hours after admission, he suffered a cardiacarrest (whether it was VF/VT or PEA is not available) and expired. The rhythm in ECG #1 is sinus tachycardia at 115-120/minute.
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Prevention of torsade depointes in hospital settings: a scientific statement from the American HeartAssociation and the American College of Cardiology Foundation. which is 0.6 So is it really prolonged?
A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospitalcardiacarrest resuscitation. Secondary outcomes included the number of post-drug defibrillations and survival to hospital discharge. This was before thrombolytics gained full use in our admitting hospital.
Vitals were reported as within normal limits except for tachycardia. Side note: I think the rhythm is probably sinus tachycardia, but I can't easily point out the sinus P waves. ( She survived the hospitalization, but long term outcome is not available. Plus recommendations from a 5-member panel on cardiacarrest.
There is sinus tachycardia with PVCs displaying various degrees of fusion ( See Ken Grauer's comment for below for a more detailed analysis of this rhythm ). If the ventricular escape rhythm also gives out, the patient has cardiacarrest. After ROSC, EKG 5 was recorded: This was interpreted as showing ventricular tachycardia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content