This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiacarrest, defibrillated, diffuse ST depression and ST Elevation in aVR.
ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiacarrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.
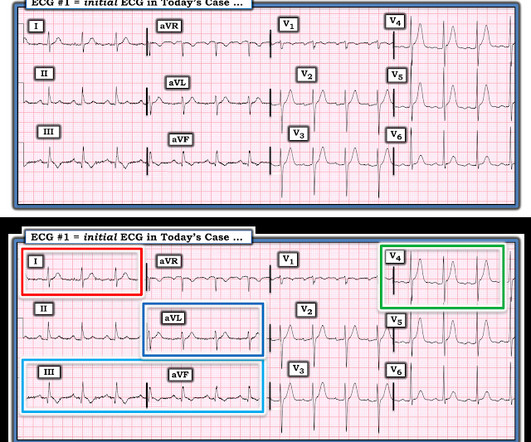
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Current Emergency and Hospital Medicine Reports (2013) 1:4352.
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardial infarction (STEMI). We compared patientlevel characteristics of patients who did and did not undergo PCI at each hospital. versus 7.4%,P<0.001), versus 5.1%,P<0.001)
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chest pain and SOB. She was diagnosed with a Non-STEMI and kept overnight for a next day angiogram.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
Past medical history included RBBB without other cardiac history, but old ECG was not available. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The patient had a protracted hospitalization and did not survive.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. On arrival, GCS was 13 and the patient complained of ongoing chest pain.
Hospital admission had been recommended, but she left that ED against medical advice. If cardiacarrest from hypokalemia is imminent (i.e., to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2
Another ECG was recorded 5 minutes later just before arrival at the hospital: Similar The patient was transported to a nearby suburban hospital with PCI capabilities while my partner cared for her. It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. From Gue at al.
He had a previous MI with cardiacarrest 2 years prior. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. The ST depression may be the most visibly obvious sign of STEMI. Some are STEMI-equivalents.
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. These studies did not address OMI ECG findings!!!
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
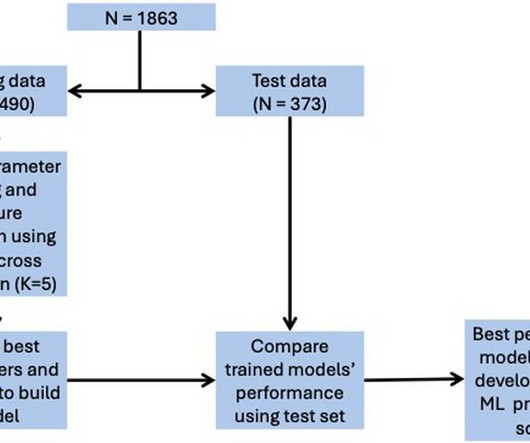
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for in-hospital mortality, 0.78 for ICU admission, and 0.74 for LVEF < 40%.
3 studied 416 patients hospitalized with COVID in China, of whom 82 had an initial cTn(I) above the upper reference limit. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. 3–8 Shi et al. Clin Chem [Internet] 2017;63(1):101–7.
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. What is the utility of a head CT in cardiacarrest?
He had multiple cardiacarrests with ROSC regained each time. He spent almost 2 months in the hospital, and reportedly made a full neurologic recovery. This patient arrested shortly after hospital arrival. As a result — the history will often be limited to what was known prior to the arrest.
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest. Is it STEMI? What does the ECG show? Also see the bizarre Bigeminy.
Discharging patients with NH-IMRangio<40 units at 48 hours after admission would reduce the total in-hospital stay by 943 days (median 2 [1–4] days per patient).CONCLUSIONS:NH-IMRangiois NH-IMRangioguided strategies to early discharge may contribute to safely shorten hospital stay, optimizing resources utilization.
link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! C harges and cost have no relation to each other in hospital billing. Am J Emerg Med 36(10):1771-1774.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient was extubated on Day-3 of the hospital stay. The stay in the cardiac intensive care unit (CICU) was further complicated by sepsis, delirium, GI bleeding, and anuric renal failure with need for renal replacement therapy.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria.
But limitation of this ST elevation to a single lead is not consistent with any distribution of a STEMI. Unfortunately — the patient abruptly developed hypoxemia, followed by cardiacarrest with PEA. It was thought that this action precipitated the patient's desaturation, and led to his cardiacarrest.
Møller, MD , professor in the Department of Cardiology at the Odense University Hospital in Denmark, consultant at the cardiac intensive care unit of Copenhagen University Hospital Rigshospitalet and the study’s lead author. “I I think this will be a routine device that will be used in these desperately ill patients.”
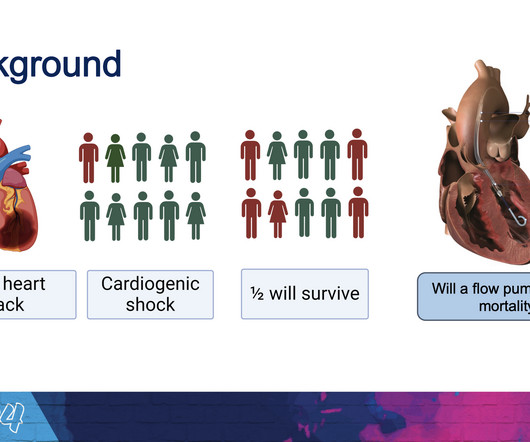
This pattern is essentially always accompanied by cardiogenic shock and high rates of VT/VF arrest, etc. Code STEMI was activated. Plus recommendations from a 5-member panel on cardiacarrest. A man in his 80s with chest pain What, besides large anterior STEMI, is so ominous about this ECG?
The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." About two hours after admission, he suffered a cardiacarrest (whether it was VF/VT or PEA is not available) and expired. The whole paradigm is literally called "STEMI" vs. "NSTEMI."
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". A few days later an ECG was repeated which showed normal sinus rhythm with no further hyperkalemia findings: After a 3-week hospitalization for acute renal failure, hyperkalemia, and compartment syndrome, the patient was discharged to acute rehab.
There is worrisome T-wave inversion in inferior leads as well, which is another clue to LAD Occlusion In fact, this ECG meets STEMI criteria!! Why does the conventional algorithm not diagnose STEMI? Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 What’s the story?"
The computer called this Acute STEMI What do you think? STEMI never has a very short QT. There is Bazett, Fridericia, Hodges, Framingham and Rautaharju -- see here at mdcalc: [link] If the ST Elevation here were due to STEMI, it would be an LAD Occlusion. Treatment is by ICD ( implantable cardioverter defibrillator ).
AimThis study aimed to protect brain functions in patients who experienced in-hospitalcardiacarrest through the application of local cerebral hypothermia. underwent emergency coronary angiography due to ST-elevation myocardial infarction (STEMI). Among the patients, 62.5%
They presented to a hospital clinic for routine paracentesis, after which they developed nausea and syncope attributed to a vasovagal episode from the procedure. 2] Curiously, ACLS does not include consideration of calcium in its bradycardia algorithm, which could have prevented the arrest and which along with the epi produced ROSC.
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospitalcardiacarrest resuscitation. The final angiographic result is very good.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content