This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Researchers at Oregon Health & Science University have found that quality of care for pediatric patients who experience cardiacarrest outside of the hospital is lower compared with adults, prompting an urgent call to action to improve care delivery for the potentially deadly event.
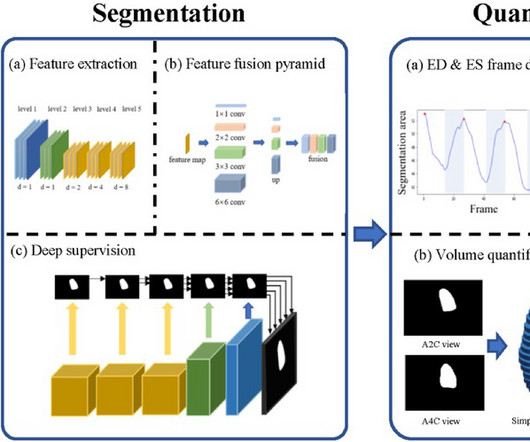
BackgroundPercutaneous extracorporeal membrane oxygenation (ECMO) is administered to pediatric patients with cardiogenic shock or cardiacarrest. Additionally, raw data images of apical 2-chamber and 4-chamber views were utilized for EF assessment via a Pediatric ECMO Quantification machine learning-enabled AI (automated-EF).ResultsThere
The impact of chest compression (CC) pause duration on survival outcomes in pediatric in-hospitalcardiacarrests remains unclear, despite the American Heart Association’s recommendation to limit pauses to less than 10 seconds for children without solid evidence. Original article: Lauridsen KG et al.
based OSF HealthCare's Childrens Hospital of Illinois became the first in the world to implant an extravascular implantable, cardioverter-defibrillator in a pediatric patient who had suffered sudden cardiacarrest. A team at Peoria, Ill.-based
Does hospital median cardiopulmonary resuscitation (CPR) duration in patients without return of circulation (ROC) predict survival among hospitalized children?
BackgroundTelecommunicator CPR (T‐CPR), whereby emergency dispatch facilitates cardiacarrest recognition and coaches CPR over the telephone, is an important strategy to increase early recognition and bystander CPR in adult out‐of‐hospitalcardiacarrest (OHCA).
BackgroundRapid recognition of pediatric outofhospital cardiacarrest (POHCA) is a critical component to prompt initiation of bystander interventions. Journal of the American Heart Association, Ahead of Print.
Understanding why ETCO2 is recommended in cardiacarrest with Swami, practical steps to organ donation in the ED with Dr. Andrew Healy, using your hospital food court to treat paraphimosis, rectal prolapse and food bolus obstruction with Dr. Sarah Foohey, QI Corner with Dr. Tahara Bhate, 4 Medicolegal Myths with Dr. Jennifer C.
Demographic, and pre-, intra-, and post-PHT clinical, brain imaging and RT (physical, occupational, speech and feeding therapy) data were collected up to PHT hospitalization. Data are presented as frequency (%) or median (Inter Quartile Range-IQR).Results:Of Additionally, 38(45%) were ischemic and 34(40%) were hemorrhagic strokes.Of
However, according to these diagnostic criteria (JACC 2011; 57(7):802), it is a Bazett corrected QT of less than 330-370, depending on other diagnostic criteria, including 1) h/o cardiacarrest, 2) sudden syncope, 3) family hx of sudden unexplained arrest at age less than 40, 4) family hx of SQTS. Some other points: 1.
BackgroundPediatric out‐of‐hospitalcardiacarrest (POHCA) is associated with significant mortality and poor neurological outcomes. The case group included children (aged 1 day to 17 years) who experienced an out‐of‐hospitalcardiacarrest between 2004 and 2020.
On this month's EM Quick Hits podcast: Stephen Freedman on pediatric bloody diarrhea, S-TEC and hemolytic uremic syndrome, Justin Morgenstern on the evidence for IM epinephrine in out of hospitalcardiacarrest, Matthew McArther on recognition and ED management of dengue fever, Andrew Petrosoniak on imaging decision making in trauma in older patients, (..)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content