This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
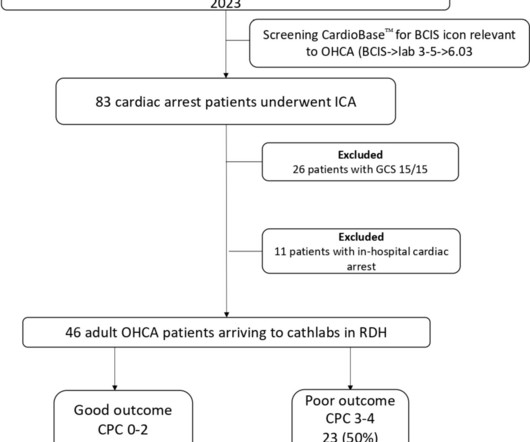
Introduction and objectives Decision-making regarding prognosticating out-of-hospitalcardiacarrest (OHCA) remains challenging at the front door. The study aims to validate the MIRACLE2 score in a district general hospital (DGH). Results A total of 46 patients satisfied the study criteria, of which 43 (93%) were males.
Objective Out-of-hospitalcardiacarrest (OHCA) is a major public health challenge across Europe, with a survival rate of only 8.5% to hospital discharge. Implementing a community first responder (CFR) system, including earlier Basic Life Support and defibrillation, can enhance survival rates and neurological outcomes.
(MedPage Today) -- Therapeutic hypothermia did not improve survival or functional outcomes in unconscious patients after out-of-hospitalcardiacarrest with initial nonshockable rhythm, a meta-analysis of patient-level data found. The primary.
has no memory of his own cardiacarrest in 2016. He only knows that first responders resuscitated his heart with a shock from a defibrillator, ultimately leading to his complete recovery and putting him among fewer than one in 10 people nationwide who survive cardiacarrest outside of a hospital.
She is healthy with no known cardiac disease. A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. The morning before the cardiacarrest potassium was 4,3.mmol,
People who experience out-of-hospitalcardiacarrest often require care at a regional center for continued treatment after resuscitation, but many do not initially present to the hospital where they will be admitted. Circulation, Ahead of Print.
An analysis of data for more than 500,000 out-of-hospitalcardiacarrests in the U.S. found key differences in outcomes between cardiacarrests caused by drug overdoses and cardiacarrests due to other causes, according to new research published today in the Journal of the American Heart Association.
BackgroundGiven increases in drug overdose‐associated mortality, there is interest in better understanding of drug overdose out‐of‐hospitalcardiacarrest (OHCA). Arrests involving patients <18 years, health care facility residents, patients with cancer diagnoses, and patients with select missing data were excluded.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. AN evaluation of efficacy amonGst cOmpression only and standard CPR) trial is designed to evaluate whether compression-only cardiopulmonary resuscitation (CPR) by trained laypersons is noninferior to standard CPR in adult out-of-hospitalcardiacarrest.
In a prospective, multicentre, parallel, randomised clinical trial titled ARREST, researchers aimed to evaluate the effectiveness of expedited transfer to a cardiacarrest center compared to standard care following out-of-hospitalcardiacarrest. The ARREST study is the first randomized trial of its kind.
BackgroundOutofhospital cardiacarrest (OHCA) with initial shockable rhythm generally has a favorable prognosis. However, the prognosis worsens when this rhythm transitions to nonshockable rhythm on hospital arrival. The primary outcome was rhythm conversion to nonshockable on hospital arrival.
The impact of chest compression (CC) pause duration on survival outcomes in pediatric in-hospitalcardiacarrests remains unclear, despite the American Heart Association’s recommendation to limit pauses to less than 10 seconds for children without solid evidence. Original article: Lauridsen KG et al.
Yet, overall survival among patients with out-of-hospitalcardiacarrest is approximately 10%, even in well-performing emergency medical systems. The interventions that are undertaken at the scene of a cardiacarrest are the most likely interventions to improve outcomes: early.
Every 10 years, the American Heart Association (AHA) Emergency Cardiovascular Care Committee establishes goals to improve survival from cardiacarrest. Circulation, Ahead of Print.
Michael's Hospital researchers shows that middle-aged men are the demographic most at risk for sudden cardiacarrest while playing sports, and there are ways to improve outcomes for people who experience a sudden cardiacarrest in public. A new study by St.
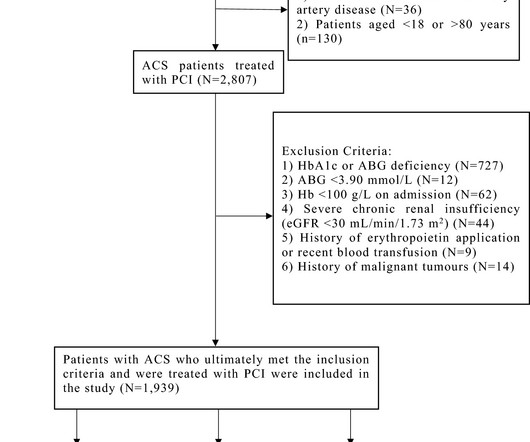
The stress hyperglycaemic ratio (SHR), a new marker that reflects the true hyperglycaemic state of patients with acute coronary syndrome (ACS), is strongly associated with adverse clinical outcomes in these pa.
Does hospital median cardiopulmonary resuscitation (CPR) duration in patients without return of circulation (ROC) predict survival among hospitalized children?
Introduction Immune checkpoint inhibitors have advanced the outcomes of many different types of cancer. years and was admitted after an out-of-hospitalcardiacarrest due to ventricular fibrillation. years and was admitted after an out-of-hospitalcardiacarrest due to ventricular fibrillation.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. Background:Prompt initiation of bystander cardiopulmonary resuscitation (CPR) is critical to survival for out-of-hospitalcardiacarrest (OHCA). Results:Of 78 048 patients with a witnessed OHCA treated with bystander CPR, the mean age was 63.5±15.7
Introduction The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (ECPR) in selected patients after out-of-hospitalcardiacarrest (OHCA) is an established method if return of spontaneous circulation cannot be achieved.
The targeted Automated External Defibrillator (AED) program in the Sao Paulo Metro has yielded promising results in improving survival rates for individuals experiencing out-of-hospitalcardiacarrest (OHCA) due to ventricular arrhythmias.
BACKGROUND:In patients with out-of-hospitalcardiacarrest who present with an initial shockable rhythm, a longer delay to the first shock decreases the probability of survival, often attributed to cerebral damage. This may explain the worse outcomes in patients with a long delay to defibrillation.
Although PAD can substantially increase the survival of cardiacarrest, PAD use remains low. The primary outcomes were the rate of bystander PAD use, sustained return of spontaneous circulation, survival to discharge, and favorable neurological outcomes. The rate of favorable neurological outcomes increased from 4.4%
BackgroundAlthough they are fastgrowing populations in the United States, little is known about survival outcomes of Hispanic and Asian patients after inhospital cardiac arrest.Methods and ResultsIn Get With The GuidelinesResuscitation, we identified Asian, Hispanic, and White adults with inhospital cardiacarrest during 2005 to 2023.
BackgroundDespite the wellknown importance of witnessed arrest and bystander cardiopulmonary resuscitation (CPR) for outofhospital cardiacarrestoutcomes, previous studies have shown significant statistical inconsistencies. The outcome measure was prehospital return of spontaneous circulation (ROSC).
In a patient-level analysis of data from two recent trials, patients with out-of-hospitalcardiacarrest and an initial nonshockable rhythm treated with hypothermia did not have increased survival or improved functional outcome compared with normothermia.
Ninety-five percent of CPR training manikins on the global market are flat-chested, possibly contributing to disproportionate survival outcomes for women after cardiacarrest, according to a study published Nov. 21 in Health Promotional International.
Background Out-of-hospitalcardiacarrest (OHCA) has a poor prognosis. In terms of outcomes assessed, our meta-analysis revealed a similar rate of all-cause mortality (pooled odds ratio [OR] 1.22 [0.99–1.50], A random effects meta-analysis was performed. 1.50], P = 0.06, I2 = 0%), neurological status (pooled OR 0.94 [0.74–1.21],
BackgroundSocial determinants of health such as residential segregation have been identified as drivers of disparities in health outcomes; however, this has been understudied for outofhospital cardiacarrest (OHCA). The primary predictor for this study was the Index of Concentration at the Extremes.
Background Data on the management of patients with cancer presenting with sudden cardiacarrest (SCA) are scarce. We aimed to assess the characteristics and outcomes of SCA according to cancer history. Results Out of 4069 patients who had SCA admitted alive in hospital, 207 (5.1%) had current or past medical history of cancer.
Background:Out-of-hospitalcardiacarrest (OHCA) is associated with unfavourable survival rates and neurological outcomes. This study aims to investigate the impact of BPV within the first 48 hours on the outcomes in patients experiencing OHCA.Methods:A retrospective analysis was conducted on data from OHCA patients.
BackgroundCoronary angiography (CAG) and targeted temperature management (TTM) may improve clinical outcomes after outofhospital cardiacarrest. We investigated the associations between the timing of interventions and whether CAG was performed before TTM initiation (CAGfirst) and good neurological outcomes.
However, few national population‐based studies have investigated the comprehensive effectiveness of those updates for out‐of‐hospitalcardiacarrest due to shockable rhythms. in 2006, and 3.01
Dynamics of rSO2 changes in the peri-resuscitation period and depending on the drugs administered have not yet been fully investigated.Hypothesis:It was assumed that continuous monitoring of rSO2 using NIRS during CPR can serve as an indicator of resuscitation quality and outcome. CPR was performed by the Early Response Team.
Background:Out-of-hospitalcardiacarrest (OHCA) typically results in low survival rates and undesirable neurological outcome. Additionally, a higher MAP level with target MAP ≥ 80 mmHg within the first 12 hours was correlated with better neurological outcomes (odd ratio [OR]: 0.370, 95% CI: 0.147-0.935, P = 0.035).Conclusions:MAP
Introduction:Over 290,000 in-hospitalcardiacarrests occur annually in the United States. Evidence supports high-quality chest compressions as a vital factor to achieving return of spontaneous circulation (ROSC) and improving outcomes after cardiacarrest.
BackgroundRisk stratification is important in patients with post–cardiacarrest syndrome. We validated the accuracy of the CAST/rCAST scores for predicting neurological outcomes at 30 days. The proportion of patients with favorable neurological outcomes was 16.6%. A total of 1135 patients were analyzed.
Background:In out-of-hospitalcardiacarrest (OHCA) patients with an initial shockable rhythm, epinephrine increases the likelihood of return of spontaneous circulation (ROSC), but its effect on neurological outcome remains uncertain. Circulation, Volume 150, Issue Suppl_1 , Page A4137905-A4137905, November 12, 2024.
Background:Different from the negative impact of COVID-19 pandemic on outcomes after out-of-hospitalcardiacarrest (OHCA) collapsed before emergency medical service (EMS) arrival, there was a report suggested that COVID-19 pandemic did not affect outcomes after OHCA witnessed by EMS personnel. to 0.08; p = 0.21).
C and hypothermia at 33°C had similar outcomes in out-of-hospital post cardiacarrest patients. Primary outcome was favorable neurological outcomes (cerebral performance categories of 1 or 2) at hospital discharge. The median age was 62 years and 105 (66%) patients had cardiac etiology.
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiacarrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? Then the patient's electronic record from an outside hospital appeared. I wrote the following note in the chart: "V Fib arrest, has ICD.
Introduction:Out-of-hospitalcardiacarrest (OHCA) remains a significant public health challenge, with conventional cardiopulmonary resuscitation (CPR) often yielding limited success. Primary efficacy outcome was defined as survival to hospital discharge, while primary safety outcome was assessed for bleeding events.
BackgroundPatients with out‐of‐hospitalcardiacarrest (OHCA) in rural areas experience longer emergency response times and have lower survival rates compared with patients in urban areas. Volunteer responders might improve care and outcomes for patients with OHCA specifically in rural areas.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content