This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundEarly coronary angiography (CAG) in post-cardiacarrest patients without ST-segment elevation is a topic of debate. A random-effects model pooled odds ratios (ORs) with 95% confidence intervals (CIs). Early CAG significantly reduced long-term mortality [OR: 0.66 (0.51–0.85)], Interpretation should be cautious.
Out-of-hospitalcardiacarrest (OHCA) mostly occurs in crowded public places outside hospitals, such as public sports facilities, airports, railway stations, subway stations, and shopping malls. ECMO support therapy for patients with cardiacarrest can be considered when economic conditions permit.
Methods Predefined casecontrol sub-study within the international Targeted Hypothermia versus Targeted Normothermia after Out-of-HospitalCardiacArrest (TTM2) trial. OHCA survivors at 8 of 61 TTM2 sites in Sweden, Denmark and the United Kingdom were invited. Participants were matched 1:1 to MI controls.
Background Out-of-hospitalcardiacarrest (OHCA) has a dismal prognosis with overall survival around 10%. Previously, 80% of sudden cardiacarrest have been attributed to coronary artery disease. Only 30% of all cases of OHCA admitted to hospital were diagnosed with AMI.
BackgroundCardiogenic shock complicating acute myocardialinfarction is associated with a high mortality rate. Cardiogenic shock after outofhospital cardiacarrest (OHCA) can be due to transient myocardial stunning but also reflect the increasing severity of ongoing heart failure.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardialinfarction (STEMI). We compared patientlevel characteristics of patients who did and did not undergo PCI at each hospital. versus 7.4%,P<0.001),
Impella and venoarterial extracorporeal membrane oxygenation (VA-ECMO) in patients with acute myocardialinfarction-related cardiogenic shock (AMICS). Impella patients were older (34% vs. 13% >75 years, p < 0.001) and less frequently presented after an out-of-hospitalcardiacarrest (18% vs. 40%, p < 0.001).
BackgroundAcute myocardialinfarction complicated by cardiogenic shock (AMI‐CS) is associated with significant morbidity and mortality. The primary end point was in‐hospital mortality. Survival rates to hospital discharge were high. Journal of the American Heart Association, Volume 12, Issue 23 , December 5, 2023.
Secondary outcomes included in-hospital and 30-day events. SMuRF-less patients were more likely to present with cardiacarrest (6.6% vs 3.9%, p<0.001) and ST-elevation myocardialinfarction (59.1% Methods We analysed data from the Melbourne Interventional Group PCI Registry. vs 9.9%, p=0.029).
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
This analysis included 17 843 admissions across 34 sites and compared interhospital tertiles of CCRx (eg, mechanical ventilation, mechanical circulatory support, continuous renal replacement therapy) utilization and its adjusted association with in-hospital survival using logistic regression.
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] Clinical characteristics of dialysis patients with acute myocardialinfarction in the United States.
Specifically, the study highlights a strong correlation between AKI and heightened complication rates, poor functional outcome, extended hospital stays, and elevated mortality rates.
Another ECG was recorded 5 minutes later just before arrival at the hospital: Similar The patient was transported to a nearby suburban hospital with PCI capabilities while my partner cared for her. It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored.
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Here is the abstract: Background Identification of ST elevation myocardialinfarction (STEMI) is critical because early reperfusion can save myocardium and increase survival.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. 3 studied 416 patients hospitalized with COVID in China, of whom 82 had an initial cTn(I) above the upper reference limit. 3–8 Shi et al.
The study utilized the ISCHEMIA primary outcome, a composite measure of cardiovascular death, protocol-defined myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiacarrest. years, with 57.1% occurring within 30 days after CABG.
Overlap propensity score weighting was performed to assess the association between transfer status and in-hospital mortality. During the hospitalization, they had higher rates of renal failure, pulmonary artery catheter use, and mechanical circulatory support use. In-hospital mortality was lower in transferred patients39.1%
If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 Literature on Hypokalemia as a risk for ventricular fibrillation in acute myocardialinfarction. mEq/L, and 10 mEq would increase it by 3.3 mEq/L, from 1.9
What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. in Vienna found that 27 of 765 (4%) of out of hospitalcardiacarrests (OHCA) were due to SAH.
There is limited understanding of race differences in the management and outcomes of CS.Methods:We queried the US National Inpatient Sample database (years 2016-2021) for CS hospitalizations in adults and categorized them by presence of acute myocardialinfarction (AMI) on admission. 0.93), pLVAD (aOR: 0.79, 95%CI: 0.72-0.86),
BACKGROUND:In patients with ST-segment–elevation myocardialinfarction complicated by cardiogenic shock, primary percutaneous coronary intervention (pPCI) is the preferred revascularization option. pharmacoinvasive and 46.2% pharmacoinvasive and 46.2% The incidence of the primary safety outcome was 10.1% 1.09];P=0.08).CONCLUSIONS:In
Background Left ventricular free-wall rupture (LVFWR) is a catastrophic complication of acute myocardialinfarction (AMI). Historically, cardiac surgery is considered the treatment of choice. The primary end-point was in-hospital morality rate; secondary outcomes were long-term survival and postoperative complications.
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for in-hospital mortality, 0.78 for ICU admission, and 0.74 for LVEF < 40%.
BackgroundPatients hospitalized with COVID19 from socioeconomically vulnerable communities are at risk for inhospital cardiovascular events. ConclusionsAmong survivors of COVID19 hospitalization, patientlevel social vulnerability was associated with cardiovascular events, explained by increased comorbidities.
Abstract Aims This study aimed to investigate incidence and predictors of weaning failure and in-hospital death after successful weaning from veno-arterial extracorporeal membrane oxygenation (VA-ECMO) in patients with cardiogenic shock (CS). Of the successfully weaned patients, 150 (36.6%) died before hospital discharge.
BACKGROUND:Patients with ST-segment–elevation myocardialinfarction but no coronary microvascular injury are at low risk of early cardiovascular complications (ECC). Discharging patients with NH-IMRangio<40 units at 48 hours after admission would reduce the total in-hospital stay by 943 days (median 2 [1–4] days per patient).CONCLUSIONS:NH-IMRangiois
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). The patient was extubated on Day-3 of the hospital stay. Over the next couple of days the patient was weaned off of mechanical circulatory support.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 Nearly 20% of those people who have had a MI will be hospitalized again within five years due to a second event.5 4 In the U.S. N Engl J Med.
Møller, MD , professor in the Department of Cardiology at the Odense University Hospital in Denmark, consultant at the cardiac intensive care unit of Copenhagen University Hospital Rigshospitalet and the study’s lead author. “I I think this will be a routine device that will be used in these desperately ill patients.”
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardialinfarction. C harges and cost have no relation to each other in hospital billing. No, again, charges and cost have no relation to each other in hospital billing. This paper was just published: Noll S. October 2018.
Other cases of LAD OMI with RBBB/LAFB: A man in his 40s who really needs you to understand his ECG CardiacArrest at the airport, with an easy but important ECG for everyone to recognize A woman in her 60s with 6 hours of chest pain, dyspnea, tachycardia, and hypoxemia Ventricular Fibrillation, ROSC after perfusion restored by ECMO, then ECG.
BackgroundDespite the increasing long‐term survival after out‐of‐hospitalcardiacarrest (OHCA), the risk of subsequent acute myocardialinfarction (AMI) remains poorly understood. Journal of the American Heart Association, Ahead of Print.
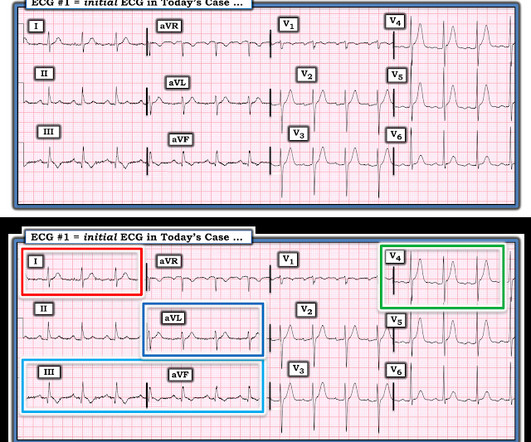
Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 Here is a case in which the ECG looks normal but not when compared to the old one. (In In this case, 4 variable formula was positive and the Queen diagnosed OMI with mid confidence). ng/ml) The sender asked: "Would you activate the cath lab?"
We evaluated the primary outcome (cardiovascular death, myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiacarrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. of invasive‐assigned women revascularized versus 81.2%
AimThis study aimed to protect brain functions in patients who experienced in-hospitalcardiacarrest through the application of local cerebral hypothermia. underwent emergency coronary angiography due to ST-elevation myocardialinfarction (STEMI). Among the patients, 62.5%
REFERENCE Prevention of primary ventricular fibrillation in acute myocardialinfarction with prophylactic lidocaine [link] Primary ventricular fibrillation (VF) during an acute myocardialinfarction (AMI) occurs with a high incidence and mortality rate with or without thrombolysis. DOI: 10.1016/j.resuscitation.2025.110515
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content