This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
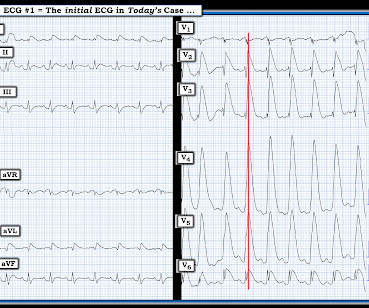
She is healthy with no known cardiac disease. A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. The morning before the cardiacarrest potassium was 4,3.mmol,
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronary artery disease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
The ECG shows severe ischemia, possibly posterior OMI. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another.
ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiacarrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.
This ECG is diagnostic of diffuse subendocardial ischemia. What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. We studied this and published the abstract below in 2010.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. He had multiple cardiacarrests with ROSC regained each time.
. = The H ISTORY in T oday's C ASE: The patient in today's case is a teenager who presented to the ED ( E mergency D epartment ) in cardiacarrest after electrocution. The "good news" — is that after an extended hospitalization, the patient was finally discharged home, and doing well. =
A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
He was intubated in the field and sedated upon arrival at the hospital. This was interpreted by the treating clinicians as not showing any evidence of ischemia. However, he did not remember much from the day of the arrest. At his family's request, he was transferred to a hospital closer to his home to continue care.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). In fact, most do not make it to the hospital alive, which explains why only a tiny percent of OMI are due to full LM occlusion.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
3 studied 416 patients hospitalized with COVID in China, of whom 82 had an initial cTn(I) above the upper reference limit. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. Cardiac troponin I in patients with coronavirus disease 2019 (COVID-19): Evidence from a meta-analysis.
The patient was extubated on Day-3 of the hospital stay. The stay in the cardiac intensive care unit (CICU) was further complicated by sepsis, delirium, GI bleeding, and anuric renal failure with need for renal replacement therapy. There is no definite evidence of acute ischemia. (ie,
If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. So there is now high pre-test probability + refractory ischemia + Modified Sgarbossa + dynamic ECG changes. VF arrest is of course "electrical instability"! Learning points 1.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
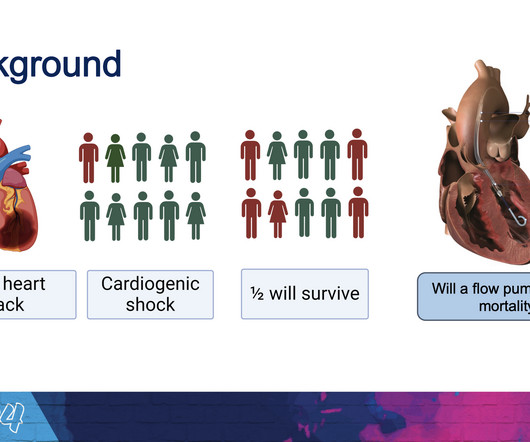
Møller, MD , professor in the Department of Cardiology at the Odense University Hospital in Denmark, consultant at the cardiac intensive care unit of Copenhagen University Hospital Rigshospitalet and the study’s lead author. “I I think this will be a routine device that will be used in these desperately ill patients.”
It should be known that each category can easily manifest the generic subendocardial ischemia pattern. In general, subendocardial ischemia is a consequence of global supply-demand mismatch that usually ameliorates upon addressing, and mitigating, the underlying cause. What’s interesting is that the ECG can only detect ischemia.
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. He could not be resuscitated.
The differential is: Posterolateral OMI or subendocardial ischemia The distinction between posterior OMI and subendocardial ischemia can be important and sometimes difficult. Ischemic ST depression includes posterior OMI and subendocardial ischemia. Her prior ECG on file is shown below: What are your next steps?
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chest pain that started while mowing the lawn. His chest pain was located in the central chest, non-radiating, and associated with diaphoresis, nausea, and vomiting.
He had a previous MI with cardiacarrest 2 years prior. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. This ECG is diagnostic of ischemia.
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). Plus recommendations from a 5-member panel on cardiacarrest.
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
A few days later an ECG was repeated which showed normal sinus rhythm with no further hyperkalemia findings: After a 3-week hospitalization for acute renal failure, hyperkalemia, and compartment syndrome, the patient was discharged to acute rehab. Steve, what do you think of this ECG in this CardiacArrest Patient?"
alone, more than 800,000 of these people are at risk of MI and for approximately 200,000 of them, this may well be their second life-threatening cardiac event. Nearly 20% of those people who have had a MI will be hospitalized again within five years due to a second event.5 4 In the U.S. 12 Colchicine, 0.5 34 Colchicine, 0.5
My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. This suggests ischemia of uncertain duration. Unfortunately, before this could be accomplished — the patient went into cardiacarrest.
Another ECG was recorded 5 minutes later just before arrival at the hospital: Similar The patient was transported to a nearby suburban hospital with PCI capabilities while my partner cared for her. It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored.
The 12-lead ECG and long lead II rhythm strip shown in Figure-1 — was obtained from a previously healthy, elderly woman who collapsed in the hospital parking lot. A series of cardiac arrhythmias were seen during the course of her resuscitation — including the interesting arrhythmia shown in the long lead II of Figure-1.
She was discharged after a short hospitalization with oncology and cardiology follow-up. At our hospital, I think all of our docs would want to place a pigtail catheter in the ED, under ultrasound guidance and not wait for cardiology to take the patient to the cath lab. A repeat POCUS showed resolution of her pericardial effusion.
We evaluated the primary outcome (cardiovascular death, myocardial infarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiacarrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. of invasive‐assigned women revascularized versus 81.2%
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content