This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The post EM Quick Hits 5 Ludwig’s Angina, Transient Monocular Vision Loss, D-dimer for PE Workup in Pregnancy, Pediatric Nasal Foreign Bodies, Trimethoprim Drug Interactions, Airway Management in CardiacArrest appeared first on Emergency Medicine Cases.
Despite the elevated mortality rates associated with high-risk pulmonary embolism (PE), this condition remains understudied. Data regarding the effectiveness and safety of invasive therapies such as venoarterial extracorporeal membrane oxygenation (VA-ECMO) in this patient population remains controversial.
Introduction:Brain injury is the main cause of death and disability post-cardiacarrest, and hypoxic-ischemic brain injury (HIBI) severity is associated with poor outcomes. Patients with MRI in the first 7 days after cardiacarrest were included. The patients with acute ischemic stroke were older (p<0.01).
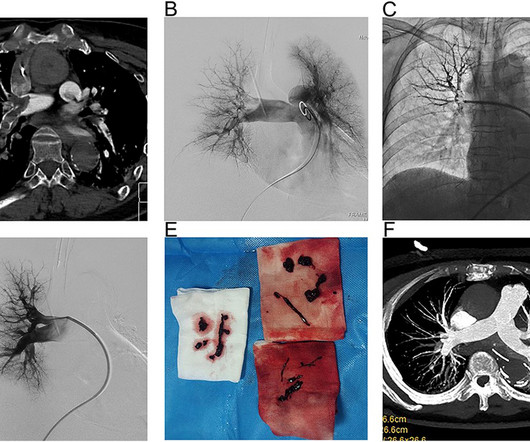
BackgroundPercutaneous mechanical thrombectomy (PMT) is increasingly used in the treatment of intermediate and high-risk acute pulmonary embolism (PE), and the treatment of high-risk PE with the aid of veno-arterial extracorporeal membrane oxygenation (VA-ECMO) has also been reported. The 12-month mortality rate was 36.4%.ConclusionVA-ECMO-assisted
High profile cases of sudden cardiacarrest in elite athletes in recent years has reminded the cardiology community of the challenging questions posed to cardiologists in these settings. Questions like: How do we prevent cardiacarrest in athletes? Can an athlete return to play after cardiacarrest?
Background Data on the management of patients with cancer presenting with sudden cardiacarrest (SCA) are scarce. Cardiac causes were less frequent among patients with cancer (mostly acute coronary syndromes, 25.5% vs 46.8%, p<0.001) and had more respiratory causes (pulmonary embolism and hypoxaemia in 34.2%
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). He had multiple cardiacarrests with ROSC regained each time. CT angiogram showed extensive saddle pulmonary embolism.
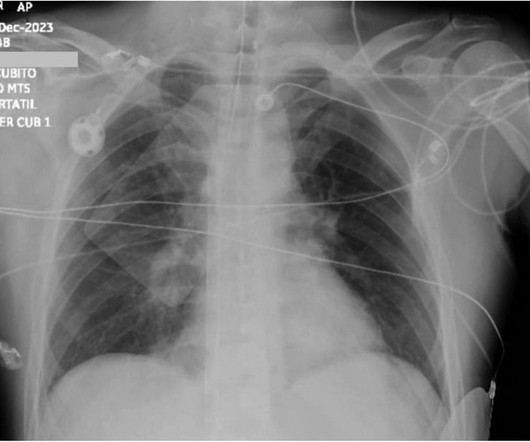
Massive pulmonary embolism (MPE) carries significant 30-day mortality and is characterized by acute right ventricular failure, hypotension, and hypoxia, leading to cardiovascular collapse and cardiacarrest.
BackgroundAcute pulmonary embolism (APE) is a common and potentially fatal cardiovascular disease that can lead to sudden cardiacarrest in severe cases. For patients with concurrent main pulmonary artery embolism and bleeding, balloon pulmonary angioplasty may be an option.
BACKGROUND:The aim of this study was to examine the impact of early versus delayed catheter-based therapies (CBTs) on clinical outcomes in patients with acute intermediate-risk pulmonary embolism (PE).METHODS:This Secondary outcomes included a composite of 30-day mortality, resuscitated cardiacarrest, and hemodynamic instability.
The post EM Quick Hits 33 Polytrauma Tips & Tricks, Toxic Megacolon, ECG in PE, Patch Calls, CT Before LP, Nebulized Ketamine appeared first on Emergency Medicine Cases.
Although one may have all kinds of ischemic findings as a result of cardiacarrest (rather than cause of cardiacarrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think?
Clinically — despite an initial 2-fold increased troponin, the normal bedside Echo was reassuring against OMI or pulmonary embolism. Smith ) — the overall impression was that ECG #1 did not suggest findings suggestive of OMI. MY Thoughts regarding ECG #2: The patient’s clinical condition worsened the next day.
This false electrical capture may have made cardiacarrest recognition difficult, and the re-arrest may have gone unrecognized for an unknown amount of time. The receiving staff suspects pulmonary embolism due to S1Q3T3 on the ECG and administers TPA. They are unable to feel a pulse and resume CPR.
Introduction The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (eCPR) has emerged as a treatment option for selected patients who are experiencing refractory cardiacarrest (CA).
Blood Clots: An enlarged heart is more prone to developing blood clots, which can lead to stroke or pulmonary embolism. CardiacArrest or Sudden Death: Cardiomegaly increases the risk of life-threatening arrhythmias, which can cause sudden cardiacarrest.
Bedside cardiac ultrasound showed moderately decreased LV function. CT of the chest showed no pulmonary embolism but bibasilar infiltrates. See this post: How a pause can cause cardiacarrest 2. She was intubated. She had an ECG recorded: This is left bundle branch block (LBBB), with appropriate proportional discordance.
This case highlights such a scenario.Case:A 75-year-old female with a history of cardiacarrest 30 years ago presented with shortness of breath and left leg swelling. She experienced massive hemoptysis, leading to respiratory and cardiacarrest, but was resuscitated. Bronchoscopy revealed clots in the left lower lobe.
Smith interpretation: This is highly likely to be due to extreme right heart strain and is nearly diagnostic of pulmonary embolism. What is the clear diagnosis and reason for arrest? It is of course pulmonary embolism. The Queen diagnosed "OMI with high confidence" due to the ST Elevation in V1-V3.
He had a cardiacarrest during the procedure and was placed back on ECMO. Another explanation is cardiac tamponade, which has also been reported to mimic MI and myocarditis. Air embolism from ECMO decannulation is another possibility, though air embolisms may include cerebrovascular pathology, which was not observed.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. CT chest showed left sided pulmonary embolism and a pulmonary infarct that had previously been mistaken for pneumonia. There was 100% proximal LAD occlusion with TIMI 0 flow, and cardiacarrest in the cath lab.
It makes pulmonary embolism (PE) very likely. First, what kind of arrest was this? It was a PEA or bradyasystolic arrest , not a shockable rhythm. Although most cardiacarrest from MI is due to ventricular fibrillation, some is due to high grade AV block, and so this could indeed be due to large acute STEMI.
Compared with 2012‐2014, the 2015‐2019 cohort showed increased odds of ICH and shock while the odds of DVT, pulmonary embolism, pneumonia, and UTI were significantly lower. Odds of a mild disability outcome increased from 16% to 20%, OR 0.65 (0.57, 0.74), while mortality decreased from 15% to 12%, OR 0.69 (0.61, 0.78).
I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. pulmonary embolism, sepsis, etc.), Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state. In non-arrest situations — escape beats and escape rhythms tend to be at least fairly regular.
However, AKI patients had higher rates of deep vein thrombosis (6.36% vs. 3.54%, p < 0.01), pulmonary embolism (4.22% vs. 1.42%, p < 0.01), pneumonia (21.39% vs. 8.84%, p < 0.01), urinary tract infection (19.07% vs. 13.32%, p < 0.01), sepsis (20.27% vs. 4.18%, p < 0.01), acute myocardial infarction (12.14% vs. 3.21%, (..)
They include myocardial ischemia, acute pericarditis, pulmonary embolism, external compression due to mass over the right ventricular outflow tract region, and metabolic disorders like hyper or hypokalemia and hypercalcemia. These are the conditions which have to be considered or excluded as they can sometimes manifest Brugada pattern on ECG.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. She was defibrillated and resuscitated. Smith: this ECG and clinical presentation is diagnostic of LAD Occlusion.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content