This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS) has been frequently documented during regional or general anesthesia. However, severe cardiacarrest induced by CAS as a result of anal-cardiac and vasovagal reflexes is relatively.
Although there is consensus on the management of patients with Brugada Syndrome with high risk for sudden cardiacarrest, asymptomatic or intermediate-risk patients present clinical management challenges. Circulation: Arrhythmia and Electrophysiology, Ahead of Print.
As a risk mitigation process, storing adequate documents for critical cases is a must. Cath Lab clinical database, in simple words, stores valuable information regarding procedures performed in a Cardiac Catheterization Lab. Documentation of critical conditions like cardiacarrest, frailty, and shock needs to be stored in real-time.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. The described rhythm was an irregular, wide complex rhythm.
The goal of this team was to improve data collection and translate identified needs from the data into resuscitation education and process improvement.Approach:The team found gaps in documentation, education, and emergency response process.
If cardiacarrest from hypokalemia is imminent (i.e., Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." mEq/L, and 10 mEq would increase it by 3.3
There is often missing documentation as to when which ECG was recorded at the time of which blood draw ( and whether any treatment had yet been initiated ). And, there is no documentation that the tachycardia has resolved. mEq/L K+ value may ( or may not ) closely correlate to the timing of today's ECG.
If cardiacarrest from hypokalemia is imminent (i.e., Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 How would you treat? mEq/L, from 1.9
While hypertension and sinus tachycardia are the most common manifestations — a variety of other tachyarrhythmias ( including VT leading to cardiacarrest ) and acute MI may be seen. Potential cardiovascular effects of acute amphetamine use are multiple. An OMI is always a possibility with acute amphetamine use.
If a patient presents with chest pain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise. CLICK HERE — for the ESC/ACC/AHA/WHF 2018 Consensus Document on the 4th Universal Definition of MI, in which these concepts are discussed and illustrated.
This patient was reported to have distant heart sounds but was not hypotensive and did not have JVD according to documentation. Beck’s triad only happens all 3 together in approximately 1/3rd of patients. Smith comment : First, IV fluids are indicated to improve preload.
The “weekend effect” is a well-documented phenomenon in hospital care, often linked to reduced staffing levels, leading to potential delays in diagnosis and intervention. Weekend procedures also face limited access to specialized cardiac teams, affecting timely decisions and making urgent procedures more difficult to schedule.
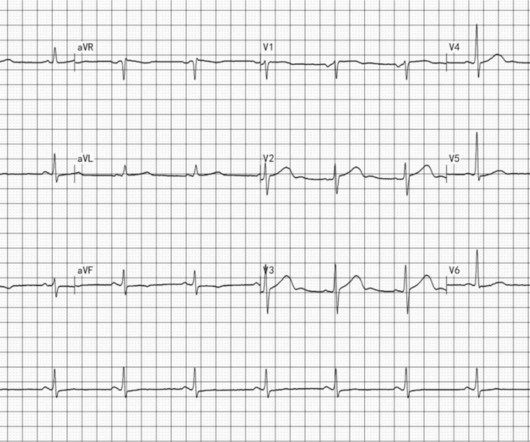
The ECG in Figure-1 was obtained from an 18-year old woman — who moments before been resuscitated from out-of-hospital cardiacarrest. Does this ECG in Figure-1 provide clue(s) to the etiology of this patient's cardiacarrest? I suspected the answer resides in the reason why an 18-year woman might have a cardiacarrest.
Patient had an unwitnessed cardiacarrest without bystander CPR performed. The crew increases this current to 75mA and documents an “improvement in patient status” with palpated pulses and a BP of 115/60. Per protocol, respirators, eye protection, and gowns were donned prior to contact. This set current is seen in Figure 5.
If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 For comparison, the same variables were reviewed for 62 consecutive patients who had transmural acute myocardial infarction (AMI) without cardiacarrest.
A few decades ago all sudden cardiacarrests with documented ventricular fibrillation (VF) and structurally normal hearts were diagnosed as idiopathic ventricular fibrillation (IVF).
ObjectiveAlthough the association between admission glucose (AG) and major adverse cardiac events (MACE) is well-documented, its relationship with 30-day MACE in patients presenting with cardiac chest pain remains unclarified.
The study documented that catheter ablation for AF in patients with heart failure was associated with a significantly lower rate of a composite endpoint of death from any cause or hospitalization for worsening heart failure, than medical therapy. 2019 Apr 2;321(13):1261-1274. doi: 10.1001/jama.2019.0693. PMID: 30874766; PMCID: PMC6450284.
In both tracings — an exceedingly fast PMVT is documented. The schematic grouping below reviews classification of PMVT types: In today's case — the sinus-conducted beats prior to and between the episode of PMVT show evidence of completed anterior wall MI. That said — there is no evidence on ECG of re-occlusion of the infarct artery.
BACKGROUND:Declining cardiovascular mortality rates have been well-documented, yet temporal trends of sudden cardiac death (SCD) in young individuals remain unclear.
Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. Drugs that have been associated with Brugada ECG patterns include tricyclic antidepressants, anesthetics, cocaine , methadone, antihistamines, electrolyte derangements, and even tramadol. [2].
Spontaneous type 1 ECG has the highest number of points at 3.5, while fever-induced type 1 ECG has 3 points. Type 2/3 ECG which gets converted to type 1 pattern with sodium channel blockers have 2 points.
Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. Drugs that have been associated with Brugada ECG patterns include tricyclic antidepressants, anesthetics, cocaine , methadone, antihistamines, electrolyte derangements, and even tramadol. [2].
On this month's EM Quick Hits podcast: Ross Prager on TEE in cardiacarrest, Justin Morgenstern on nebulized ketamine for analgesia in the ED, Hans Rosenberg & Krishin Yadav on standardizing cellulitis management, Mathew McArther on latest studies on subcutaneous insulin protocols in DKA, Jennifer C.
They increase the risk of hypertension, coronary artery disease, coronary vasospasm, arrhythmias, cardiomyopathy, cardiacarrest, and stroke. Introduction:Cocaine and methamphetamine, stimulants with potent central nervous system effects, are known to be cardiotoxic.
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. Further history later: This patient personally has no further high risk features (syncope / presyncope), but her mother had sudden cardiacarrest in sleep.
Unexplained cardiacarrest or documented VF/polymorphic VT: +3 3. Unexplained sudden cardiac death (3 categories) (+0.5 - +2) 4. Cardiacarrest. Clinical History 2.a. of atrial fib/flutter at age less than 30: +0.5 syncope of unclear etiology: +1 2.c. Suspected arrhythmic syncope: +2 2.d. Family History 3.a.
If the ventricular escape rhythm also gives out, the patient has cardiacarrest. He suffered another cardiacarrest in the ICU with ROSC after another dose of epinephrine and one round of CPR. After discussion with the patients family, the decision was made not to resuscitate in the event of re-arrest.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content