This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5.
The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Polymorphic ventricular tachycardia can be ischemic, catecholaminergic or related to QT prolongation. Cardiacarrest was called and advanced life support was undertaken for this patient. Without an MRI, it is impossible to know.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. They started CPR.
Cingolani, director of Cardiogenetics and Preclinical Research in the Department of Cardiology in the Smidt Heart Institute at Cedars-Sinai, is exploring new ways to help patients with ventricular tachycardia (VT), a recurring, abnormally fast and irregular heartbeat that starts in the lower chambers, or ventricles, of the heart.
This is obviously severe hyperkalemia and the patient is near cardiacarrest. There was no IV access, so we obtained intraosseous (IO) access, but she arrested before we could give her all the calcium. Hyperkalemia and CardiacArrest Could you have prevented this young man's cardiacarrest?
He developed cardiacarrest shortly after the ECG in Figure-1 was recorded. IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. What is the most likely cause of this arrhythmia?
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation.
See this post: How a pause can cause cardiacarrest 2. Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction. Even with tachycardia and a paced QRS duration of ~0.16
We have recently reported that chronic kidney disease (CKD) is associated with higher likelihood of sudden cardiacarrest (SCA) presenting with non-shockable rhythms (NSR) (pulseless electrical activity/asystole), as opposed to shockable rhythms (ventricular fibrillation/pulseless ventricular tachycardia).
We sought to determine predictors of RV pacing in patients who did not have a pacing indication at the time of initial ICD implant. Conclusions This study provides insight into predictors of RV pacing in ICD recipients without pacing needs at baseline.
A 60-something woman presented after a witnessed cardiacarrest. She was never defibrillated. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Cardiac cath showed minimal disease. She recovered.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. He had multiple cardiacarrests with ROSC regained each time. This patient arrested shortly after hospital arrival. CPR was initiated immediately. Initial ROSC was obtained, during which this ECG was obtained: What do you think?
She underwent cardiopulmonary resuscitation for VT/VFib — with ROSC ( R eturn O f S pontaneous C irculation ) following defibrillation and treatment with Epinephrine and Amiodarone. A series of cardiac arrhythmias were seen during the course of her resuscitation — including the interesting arrhythmia shown in the long lead II of Figure-1.
Although one may have all kinds of ischemic findings as a result of cardiacarrest (rather than cause of cardiacarrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think?
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. She was successfully revived after several rounds of ACLS including defibrillation and amiodarone.
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Should you activate the cath lab?
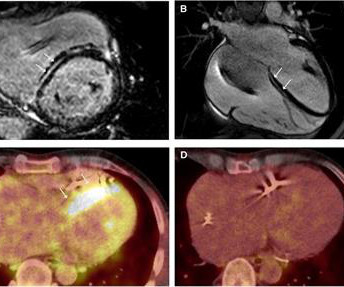
Cardiac sarcoidosis (CS), a rare condition characterized by non-caseating granulomas, can manifest with symptoms such as atrioventricular block and ventricular tachycardia (VT), as well as mimic inherited cardiomyopathies. An endomyocardial biopsy (EMB) confirmed the diagnosis of cardiac sarcoidosis.
BACKGROUND:In severely affected patients with catecholaminergic polymorphic ventricular tachycardia, beta-blockers are often insufficiently protective. The primary end point was AEs, defined as sudden cardiac death, sudden cardiacarrest, appropriate implantable cardioverter defibrillator shock, and arrhythmic syncope.
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). He required multiple defibrillations within a period of a few hours. An ICD ( Implantable Cardioverter Defibrilator ) was placed prior to discharge. What do you think?
The arrhythmia spontaneously converted before defibrillation was achieved. This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent! Complete LMCA occlusion is associated with clinical shock and/or cardiacarrest.
At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. If cardiacarrest from hypokalemia is imminent (i.e.,
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. AI recognizing cardiacarrests in emergency calls. Recently, hospitals have failed to identify 25% of cases of cardiacarrest.
Is it ventricular tachycardia (VT) due to hyperK or is it a supraventricular rhythm with hyperK? Here are other posts on hyperK, large calcium doses for hyperK, and ventricular tachycardia in hyperK Weakness, prolonged PR interval, wide complex, ventricular tachycardia Very Wide and Very Fast, What is it? How would you treat?
I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed. MY Thoughts on ECG #1: The rhythm is sinus tachycardia at 105-110/minute.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. She was ventilated by bag-valve-mask by EMS on arrival and was quickly intubated with etomidate and succinylcholine. A rectal temperature was obtained which read 107.9
Written by Pendell Meyers, with edits by Steve Smith Thanks to my attending Nic Thompson who superbly led this resuscitation We received a call that a middle aged male in cardiacarrest was 5 minutes out. There is a regular, wide complex, (mostly) monomorphic tachycardia. He was estimated to be in his 50s, with no known PMHx.
A 65 yo woman had felt ill for 36 hours, had seen her MD but without undergoing a cardiac evaluation. After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. Exact rhythm during arrest is uncertain. She collapsed and 911 was called; she was found pulseless. These patients may survive.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. There is sinus tachycardia at ~115/minute.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content