This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
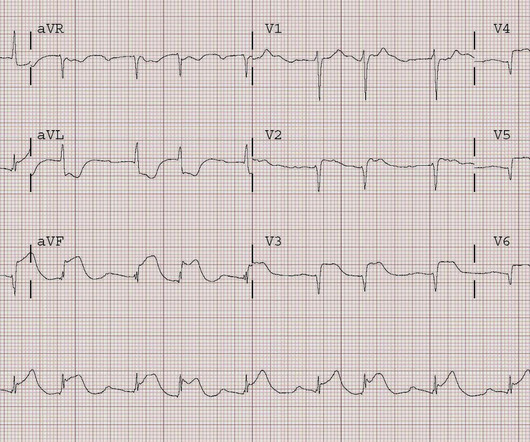
A 50-year-old woman with dextrocardia and D-transposition of the great arteries presented with a “RV defib lead impedance” remote-monitoring alert from her implantable cardioverter defibrillator (ICD). In 2012, she had a ventricular fibrillation cardiacarrest. An epicardial pacemaker was implanted.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest.
She was defibrillated successfully from ventricular fibrillation and developed a perfusing rhythm. Pressors were required, and the patient was transported to the cath lab with a door to balloon time of 60 minutes, where a proximal dominant RCA occlusion was opened and stented. She was intubated.
The patient had 2 ventricular fibrillation arrests during transport, but was immediately defibrillated both times, and was awake in the ED, when the following ECG was recorded: The ST elevation has mostly resolved on this ECG, and were it not for the arrest and the prehospital ECG, this would not be a slam dunk diagnosis.
February 2024 FDA Approvals: Innovations in Cardiovascular Interventions XACT Carotid Stent System (Approved: 02/07/2024) This approval expands the indications to be used during a Transcarotid Artery Revascularization (TCAR) procedure to prevent future strokes.
At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. This was stented. If cardiacarrest from hypokalemia is imminent (i.e., He was given amiodarone and lidocaine load and drip and K and Mg drips.
In the ambulance during transport, the patient suddenly suffered VF arrest. He was defibrillated immediately and had return of normal mental status. Given the VF arrest during transport, however, they appropriately all agreed that cath should happen sooner rather than later. They took him almost immediately for catheterization.
After the second defibrillation the patient had an organized rhythm: Bradycardic escape/agonal rhythm, with large ST deviations. The patient was taken back to the cath lab, where 100% proximal in-stent rethrombosis was found and treated. It should have been shocked at least 10 seconds ago. This is diagnostic of re-occlusion.
He was sent back to the waiting room, where he suffered a VF arrest. Defibrillation was performed, and ROSC was achieved. Smith comment: The patient was lucky to have a cardiacarrest. Total proximal LAD occlusion was found and stented at angiography soon after the ECG above.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content