This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. See my discussion at the bottom. --And
Written by Pendell Meyers A man in his 50s was found by his family in cardiacarrest of unknown duration. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. They started CPR.
ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiacarrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.
She was never seen to be in ventricular fibrillation and was never defibrillated. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. What is the utility of a head CT in cardiacarrest?
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. see below).
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
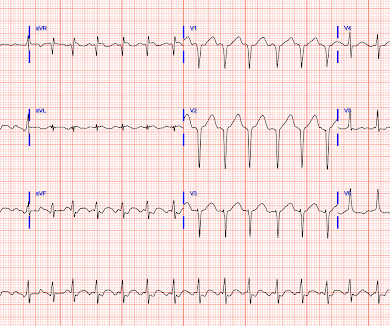
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI.
He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. Thus, this patient had increased ST elevation (current of injury) superimposed on the ST elevation of LVH and simulating STEMI. This young male had ventricular fibrillation during a triathlon. His initial ECG is shown here. He awoke and did well.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. There is atrial fibrillation.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. He had multiple cardiacarrests with ROSC regained each time. This patient arrested shortly after hospital arrival. As a result — the history will often be limited to what was known prior to the arrest.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
RBBB in acute STEMI has a very high mortality. Were it not for this prehospital ECG and the cardiacarrest, the diagnosis may have been significantly delayed. Had this happened, the artery may have re-occluded prior to angiography, with resultant recurrent cardiacarrest and/or shock and death.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. The below ECG was recorded. What do you think?
The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiacarrest. He was defibrillated. Anterolateral STEMI. The formula results in 23.43, just above the 23.4 Here is his post resuscitation ECG: Now the diagnosis is obvious.
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. The case was reviewed by all parties, and it was stated correctly that the ECG does not meet the STEMI criteria. In the ambulance during transport, the patient suddenly suffered VF arrest.
If it is STEMI, it would have to be RBBB with STEMI. This ECG pattern may be diagnostic of B rugada S yndrome IF seen in association with: i ) a history of cardiacarrest; polymorphic VT; or of non-vagal syncope; and / or ii ) a positive family history of sudden death at an early age; and / or iii ) a similar ECG in relatives.
If cardiacarrest from hypokalemia is imminent (i.e., to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 How would you treat? If the patient is at 1.8, that will raise it to 5.1
After the second defibrillation the patient had an organized rhythm: Bradycardic escape/agonal rhythm, with large ST deviations. A repeat ECG was done: Obvious anterolateral wall STEMI. It should have been shocked at least 10 seconds ago. Beats 4, 6, and 7 are narrow, as the rhythm is trying to resume from above the ventricles.
She was defibrillated and resuscitated. It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. I need to innoculate you against the subsequent opinions below.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
A 65 yo woman had felt ill for 36 hours, had seen her MD but without undergoing a cardiac evaluation. After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. Exact rhythm during arrest is uncertain. There is also ST depression in precordial leads, greatest in V3 and V4, concerning for posterior STEMI.
The computer called this Acute STEMI What do you think? STEMI never has a very short QT. There is Bazett, Fridericia, Hodges, Framingham and Rautaharju -- see here at mdcalc: [link] If the ST Elevation here were due to STEMI, it would be an LAD Occlusion. Treatment is by ICD ( implantable cardioverter defibrillator ).
Further history later: This patient personally has no further high risk features (syncope / presyncope), but her mother had sudden cardiacarrest in sleep. Implantable Cardioverter-Defibrillator ), with long-term potential for device-related complications from the ICD, including inappropriate shocks? And another finding.
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! He was sent back to the waiting room, where he suffered a VF arrest. Defibrillation was performed, and ROSC was achieved. Smith comment: The patient was lucky to have a cardiacarrest.
A 12-lead was recorded, showing "STEMI," but is unavailable. The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content