This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A new observational study suggests the position in which responders initially place the two defibrillator pads on the body may make a significant difference in returning spontaneous blood circulation after shock from a defibrillator.
has no memory of his own cardiacarrest in 2016. He only knows that first responders resuscitated his heart with a shock from a defibrillator, ultimately leading to his complete recovery and putting him among fewer than one in 10 people nationwide who survive cardiacarrest outside of a hospital.
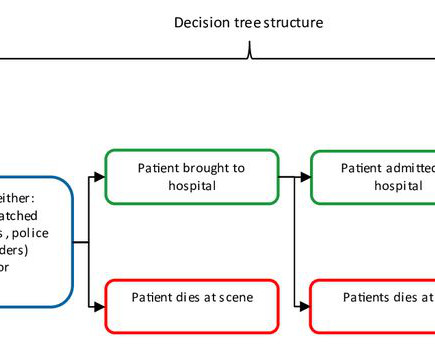
Objective Out-of-hospital cardiacarrest (OHCA) is a major public health challenge across Europe, with a survival rate of only 8.5% Implementing a community first responder (CFR) system, including earlier Basic Life Support and defibrillation, can enhance survival rates and neurological outcomes. to hospital discharge.
Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. She spontaneously converted (Defibrillation was not performed). The morning before the cardiacarrest potassium was 4,3.mmol,
It is well known that acting quickly in the event of a cardiacarrest is important, but what does a quick initial shock with a defibrillator mean exactly for patients' chances of survival?
Most cases of cardiacarrest during sport are likely to be preventable. In addition, the emergency response with cardiopulmonary resuscitation (CPR) and defibrillators within the sports context can be improved. This has been shown in a thesis from the University of Gothenburg.
Because athletes young and old can suffer cardiacarrest, some states have mandated the placement of automated external defibrillators (AEDs) in gyms, stadiums and other sports venues. But a new study finds the use of AEDs by bystanders for cardiacarrest at athletic sites didn't improve much after states enacted these laws.
Because athletes young and old can suffer cardiacarrest, some states have mandated the placement of automated external defibrillators (AEDs) in gyms, stadiums and other sports venues. But a new study finds the use of AEDs by bystanders for cardiacarrest at athletic sites didn't improve much after states enacted these laws.
The post Ep 169 CardiacArrest Controversies – Chest Compressions, Dual Defibrillation, Medications and Airway appeared first on Emergency Medicine Cases.
The targeted Automated External Defibrillator (AED) program in the Sao Paulo Metro has yielded promising results in improving survival rates for individuals experiencing out-of-hospital cardiacarrest (OHCA) due to ventricular arrhythmias. Circulation, Volume 150, Issue Suppl_1 , Page ASu505-ASu505, November 12, 2024.
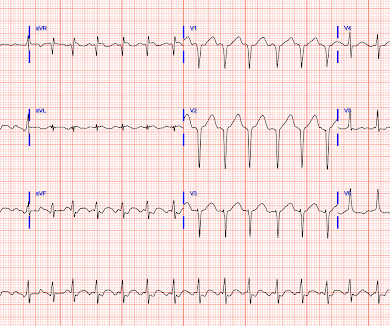
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. They started CPR.
Written by Pendell Meyers A man in his 50s was found by his family in cardiacarrest of unknown duration. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation.
In this CritCases blog Michael Misch takes us through a case of accidental hypothermia and cardiacarrest, reviewing the controversies in management as well as the guidelines for rewarming, the role of ECMO and the alterations to ACLS cardiacarrest medications, CPR and defibrillations.
Every 10 years, the American Heart Association (AHA) Emergency Cardiovascular Care Committee establishes goals to improve survival from cardiacarrest. Circulation, Ahead of Print.
ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiacarrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation.
This is obviously severe hyperkalemia and the patient is near cardiacarrest. There was no IV access, so we obtained intraosseous (IO) access, but she arrested before we could give her all the calcium. Hyperkalemia and CardiacArrest Could you have prevented this young man's cardiacarrest?
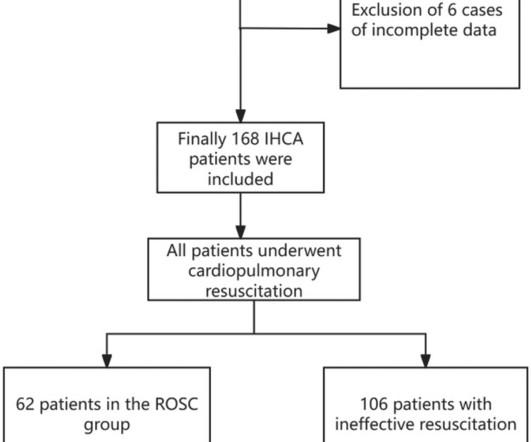
BackgroundIn-hospital cardiacarrest (IHCA) refers to the occurrence of cardiacarrest in hospitalized patients requiring chest compressions and/or defibrillation, with only about one-third of patients achieving return of spontaneous circulation (ROSC) after cardiopulmonary resuscitation.
Out-of-hospital cardiacarrest (OHCA) mostly occurs in crowded public places outside hospitals, such as public sports facilities, airports, railway stations, subway stations, and shopping malls. ECMO support therapy for patients with cardiacarrest can be considered when economic conditions permit.
(MedPage Today) -- Not all defibrillator pad positions may work equally well for patients with shockable out-of-hospital cardiacarrest. JAMA Network Open) Medical therapy for aortic stenosis? Early clinical data on evogliptin were disappointing.
(MedPage Today) -- The Jewel patch-wearable cardioverter-defibrillator delivered successful shocks for protection from sudden cardiacarrest, and people were highly compliant to wearing the water-resistant device. Journal of the American College.
BACKGROUND:In patients with out-of-hospital cardiacarrest who present with an initial shockable rhythm, a longer delay to the first shock decreases the probability of survival, often attributed to cerebral damage. Delay to first shock was defined as the time from initial emergency call until the first shock by any defibrillator.
This is the first ever video podcast on EM Cases with Jordan Chenkin from EMU Conference 2017 discussing how to optimize three aspects of cardiacarrest care: persistent ventricular fibrillation, optimizing pulse checks and PEA arrest, with code team videos contrasting the ACLS approach to an optimized approach.
BackgroundPublic access defibrillation (PAD) programs have been implemented globally over the past decade. Although PAD can substantially increase the survival of cardiacarrest, PAD use remains low. Compared with the before‐run‐in group, the rate of successful automated external defibrillator acquisition was 13.5%
BackgroundA volunteer responder program to outofhospital cardiacarrest (OHCA) was implemented stepwise in Denmark (20172020). Our results indicate successful recruitment of volunteer responders and deployment of AEDs with great potential for improving bystander defibrillation.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR. The QRS is extremely wide.
Background:Most out-of-hospital cardiacarrest (OHCA) patients who are initially treated with an automated external defibrillator (AED) and present in a non-shockable rhythm never receive a shock. The AEDs were the first defibrillator on scene either in home, in public access or by a BLS team.
Bystander use of automated external defibrillators (AEDs) can improve survival from sudden cardiacarrest (SCA), but utilization remains extremely low, attributable in part to poor access. We hypothesized that AED placement and utilization can be facilitated by identifying SCA event high-density areas in the community.
BackgroundDespite the wellknown importance of witnessed arrest and bystander cardiopulmonary resuscitation (CPR) for outofhospital cardiacarrest outcomes, previous studies have shown significant statistical inconsistencies. The W+B+ group exhibited the highest prehospital ROSC rate (14.0%).
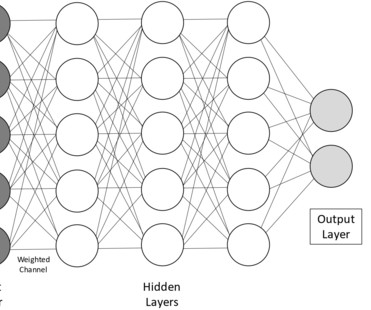
Automated external defibrillators (AEDs) and implantable cardioverter defibrillators (ICDs) are used to treat life-threatening arrhythmias. AEDs and ICDs use shock advice algorithms to classify ECG tracings as shockable or non-shockable rhythms in clinical practice.
Hypertrophic cardiomyopathy (HCM) predisposes patients to cardiacarrest (CA). While established major risk factors may warrant the need for primary prevention by implantable cardioverter-defibrillator (ICD), it is unknown if specific electrocardiographic predictors increase the risk of CA.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest.
In part due to advances in guideline-directed medical therapy (GDMT) and availability of implantable cardioverter-defibrillators (ICDs), cardiacarrest (CA) rates among patients with heart Failure (HF) decreased in the early 2000s. Relatively little is known about trends in CA associated with HF over the past decade.
We have recently reported that chronic kidney disease (CKD) is associated with higher likelihood of sudden cardiacarrest (SCA) presenting with non-shockable rhythms (NSR) (pulseless electrical activity/asystole), as opposed to shockable rhythms (ventricular fibrillation/pulseless ventricular tachycardia).
BackgroundQuantitative ventricular fibrillation (VF) analysis has the potential to optimize defibrillation by predicting shock outcomes, but its performance remains unsatisfactory. Ten features and 10 parameters were obtained from the recorded VF and defibrillation waveforms. Journal of the American Heart Association, Ahead of Print.
An Implantable cardiacdefibrillator (ICD) is recommended for primary and secondary prevention of cardiacarrest from fast ventricular arrhythmias. Patients with an ICD often have limited knowledge about end-of-life (EOL) ICD management options, and many approach the final stages of life with active shock therapy.
A 60-something woman presented after a witnessed cardiacarrest. She was never defibrillated. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Cardiac cath showed minimal disease. She recovered.
-based OSF HealthCare's Childrens Hospital of Illinois became the first in the world to implant an extravascular implantable, cardioverter-defibrillator in a pediatric patient who had suffered sudden cardiacarrest.
Therapy with implantable cardioverter-defibrillators (ICD) for secondary prevention after cardiacarrest with shockable rhythm in the absence of a reversible cause has a Class I recommendation in US guidelines. Contemporary rates of ICD use in this population are not well described.
A 50-year-old woman with dextrocardia and D-transposition of the great arteries presented with a “RV defib lead impedance” remote-monitoring alert from her implantable cardioverter defibrillator (ICD). In 2012, she had a ventricular fibrillation cardiacarrest. An epicardial pacemaker was implanted.
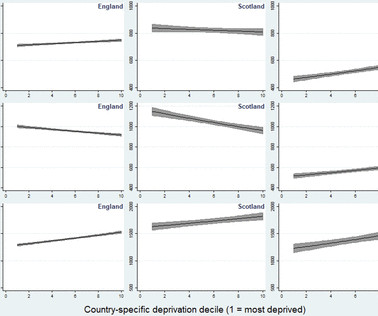
Objective The early use of automated external defibrillators (AEDs) improves outcomes in out-of-hospital cardiacarrest (OHCA). We investigated AED access across Great Britain (GB) according to socioeconomic deprivation.
BackgroundPatients with out‐of‐hospital cardiacarrest (OHCA) in rural areas experience longer emergency response times and have lower survival rates compared with patients in urban areas. Bystander defibrillation was more common in suburban areas (OR, 1.53 [95% CI, 1.02–2.31]), 3.53]) and suburban areas (OR, 2.05 [95% CI, 1.56–2.69])
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content