This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. A bedside cardiac ultrasound was normal, with no effusion. A bedside cardiac ultrasound was normal, with no effusion. An elevated troponin in a COVID patient confers about 4x the risk of mortality than a normal one.
We evaluated the association between social vulnerability and a composite of myocardialinfarction, stroke, heart failure, venous thromboembolism, cardiogenic shock, cardiacarrest, and death, following discharge, using Cox regression models.
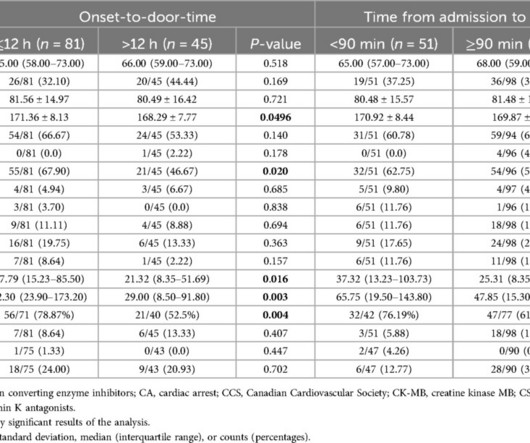
p=0.025), in the COVID-19 pandemic group of STEMI patients, compared to the pre-pandemic subset. We also observed an increase in in-hospital mortality (7.85% vs. 14.09%, p=0.033) and incidence of cardiogenic shock/cardiacarrest (16.62% vs. 26.85%, p=0.009). vs. median 5h; IQR 2.024.0, vs. median 115.0; IQR 73.0233.0,
Clinical questions : Is this an occlusion myocardialinfarction and does the patient need the cath lab? Prominent J waves and ventricular fibrillation caused by myocarditis and pericarditis after BNT162b2 mRNA COVID-19 vaccination. Internat J Arrhyth 2020 Uesako H, Fukikawa H, Hashimoto S, et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content