This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
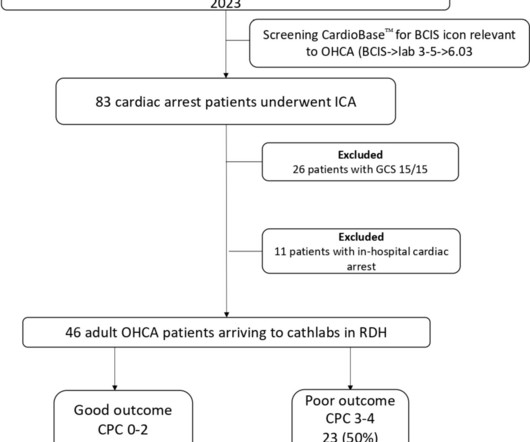
Introduction and objectives Decision-making regarding prognosticating out-of-hospital cardiacarrest (OHCA) remains challenging at the front door. The primary outcome was poor neurological recovery at hospital discharge, and the secondary outcome included poor neurological recovery at 6 months.
A new observational study suggests the position in which responders initially place the two defibrillator pads on the body may make a significant difference in returning spontaneous blood circulation after shock from a defibrillator.
Circulation, Ahead of Print. People who experience out-of-hospital cardiacarrest often require care at a regional center for continued treatment after resuscitation, but many do not initially present to the hospital where they will be admitted.
Circulation, Ahead of Print. Every 10 years, the American Heart Association (AHA) Emergency Cardiovascular Care Committee establishes goals to improve survival from cardiacarrest.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. AN evaluation of efficacy amonGst cOmpression only and standard CPR) trial is designed to evaluate whether compression-only cardiopulmonary resuscitation (CPR) by trained laypersons is noninferior to standard CPR in adult out-of-hospital cardiacarrest.
In a prospective, multicentre, parallel, randomised clinical trial titled ARREST, researchers aimed to evaluate the effectiveness of expedited transfer to a cardiacarrest center compared to standard care following out-of-hospital cardiacarrest. The ARREST study is the first randomized trial of its kind.
The impact of chest compression (CC) pause duration on survival outcomes in pediatric in-hospital cardiacarrests remains unclear, despite the American Heart Association’s recommendation to limit pauses to less than 10 seconds for children without solid evidence. Original article: Lauridsen KG et al.
BackgroundOutofhospital cardiacarrest (OHCA) with initial shockable rhythm generally has a favorable prognosis. The primary outcome was rhythm conversion to nonshockable on hospital arrival. patients achieved return of spontaneous circulation, 32.8% Journal of the American Heart Association, Ahead of Print.
Circulation, Volume 150, Issue Suppl_1 , Page ASu505-ASu505, November 12, 2024. The targeted Automated External Defibrillator (AED) program in the Sao Paulo Metro has yielded promising results in improving survival rates for individuals experiencing out-of-hospital cardiacarrest (OHCA) due to ventricular arrhythmias.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. Background:Prompt initiation of bystander cardiopulmonary resuscitation (CPR) is critical to survival for out-of-hospital cardiacarrest (OHCA).
Circulation, Volume 150, Issue Suppl_1 , Page A4141869-A4141869, November 12, 2024. Introduction:Over 290,000 in-hospital cardiacarrests occur annually in the United States. Other performance-based quality metrics to improve clinical outcomes should be included in future research with consideration of co-morbidities.
BackgroundDespite the wellknown importance of witnessed arrest and bystander cardiopulmonary resuscitation (CPR) for outofhospital cardiacarrestoutcomes, previous studies have shown significant statistical inconsistencies. The outcome measure was prehospital return of spontaneous circulation (ROSC).
Introduction The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (ECPR) in selected patients after out-of-hospital cardiacarrest (OHCA) is an established method if return of spontaneous circulation cannot be achieved.
Circulation, Ahead of Print. BACKGROUND:In patients with out-of-hospital cardiacarrest who present with an initial shockable rhythm, a longer delay to the first shock decreases the probability of survival, often attributed to cerebral damage. This may explain the worse outcomes in patients with a long delay to defibrillation.
Does hospital median cardiopulmonary resuscitation (CPR) duration in patients without return of circulation (ROC) predict survival among hospitalized children?
Although PAD can substantially increase the survival of cardiacarrest, PAD use remains low. The primary outcomes were the rate of bystander PAD use, sustained return of spontaneous circulation, survival to discharge, and favorable neurological outcomes. Journal of the American Heart Association, Ahead of Print.
BackgroundAlthough they are fastgrowing populations in the United States, little is known about survival outcomes of Hispanic and Asian patients after inhospital cardiac arrest.Methods and ResultsIn Get With The GuidelinesResuscitation, we identified Asian, Hispanic, and White adults with inhospital cardiacarrest during 2005 to 2023.
Circulation, Volume 150, Issue Suppl_1 , Page ASu1202-ASu1202, November 12, 2024. C and hypothermia at 33°C had similar outcomes in out-of-hospital post cardiacarrest patients. Primary outcome was favorable neurological outcomes (cerebral performance categories of 1 or 2) at hospital discharge.
Circulation, Volume 150, Issue Suppl_1 , Page ASa1108-ASa1108, November 12, 2024. Background:Patients with diabetes have lower survival and worse neurological outcome after cardiopulmonary resuscitation (CPR) compared with non-diabetes. Previous studies have mentioned the aberrant autophagy in diabetic mice.
Circulation, Volume 150, Issue Suppl_1 , Page A4142374-A4142374, November 12, 2024. Background:Out-of-hospital cardiacarrest (OHCA) typically results in low survival rates and undesirable neurological outcome. MAP levels were measured within the first 12 hours.
Circulation, Volume 150, Issue Suppl_1 , Page ASa505-ASa505, November 12, 2024. Once ROSC was obtained rSO2 and EtCO2 monitoring were continued for 24 hours or until cardiacarrest resumed. Introduction:The effectiveness of cardiopulmonary resuscitation is dependent on maintaining optimal cerebral perfusion.
Circulation, Volume 150, Issue Suppl_1 , Page A4137905-A4137905, November 12, 2024. Background:In out-of-hospital cardiacarrest (OHCA) patients with an initial shockable rhythm, epinephrine increases the likelihood of return of spontaneous circulation (ROSC), but its effect on neurological outcome remains uncertain.
Circulation, Volume 150, Issue Suppl_1 , Page ASa907-ASa907, November 12, 2024. However, no large-scale studies have examined the impact of COVID-19 pandemic after EMS-witnessed OHCA, focusing on favorable neurological outcomes.Research Questions:Does COVID-19 pandemic affect favorable neurological outcomes after EMS-witnessed OHCA?Aims:To
Circulation, Ahead of Print. The critical care management of patients after cardiacarrest is burdened by a lack of high-quality clinical studies and the resultant lack of high-certainty evidence. Critical care management is crucial in patients after cardiacarrest and affects outcome.
Circulation, Volume 150, Issue Suppl_1 , Page A4137065-A4137065, November 12, 2024. Introduction:Out-of-hospital cardiacarrest (OHCA) remains a significant public health challenge, with conventional cardiopulmonary resuscitation (CPR) often yielding limited success. and Revman 5.4.Results:Four to 23.28, I2: 63%).
Circulation: Cardiovascular Interventions, Volume 18, Issue 1 , Page e014499, January 1, 2025. BACKGROUND:The aim of this study was to examine the impact of early versus delayed catheter-based therapies (CBTs) on clinical outcomes in patients with acute intermediate-risk pulmonary embolism (PE).METHODS:This days;P=0.046).
Circulation, Volume 150, Issue Suppl_1 , Page A4118341-A4118341, November 12, 2024. Background:Opioid use has increased significantly in the past few decades, impacting cardiac and non-cardiac patients. p=0.35) and cardiacarrest (aOR 1.05, 95% CI 0.8 - 1.36, p=0.74) in patients on chronic opioids.
Circulation, Volume 150, Issue Suppl_1 , Page A4113864-A4113864, November 12, 2024. They had more inpatient complications including ventricular fibrillation and cardiacarrest (p <0.001) with longer mean lengths of stay (7 days vs. 5 days, p <0.001) and 30-day readmissions (28% vs. 22%, p<0.001).
Massive pulmonary embolism (MPE) carries significant 30-day mortality and is characterized by acute right ventricular failure, hypotension, and hypoxia, leading to cardiovascular collapse and cardiacarrest. Veno-venous ECMO can support oxygenation but is not designed to help circulation.
Circulation: Heart Failure, Ahead of Print. Patient characteristics, outcomes, and procedural volume were compared among 3 cohorts: admissions to non-ATCs, admissions to ATCs, and transfers to ATCs. A secondary analysis evaluated outcomes for severe HF hospitalizations (cardiogenic shock, cardiacarrest, and mechanical ventilation).
Circulation, Volume 150, Issue Suppl_1 , Page A4147424-A4147424, November 12, 2024. Prospective studies would be required to further examine the cardiovascular outcome in this cohort. Prospective studies would be required to further examine the cardovascular outcomes in this cohort.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. Admissions to CICUs with the highest tertile of CCRx utilization had a greater burden of comorbidities, had more diagnoses of ST–elevation myocardial infarction, cardiacarrest, or cardiogenic shock, and had higher Sequential Organ Failure Assessment scores.
Circulation, Volume 150, Issue Suppl_1 , Page ASu104-ASu104, November 12, 2024. Background:The incidence of cardiacarrest (CA) increases with age, leading to poorer neurological outcomes after the return of spontaneous circulation (ROSC) in the elderly.
Circulation, Volume 150, Issue Suppl_1 , Page A4134590-A4134590, November 12, 2024. Background:Despite the role of cardiac catheterization for hemodynamic assessment and endomyocardial biopsy (EMB) in children with cardiomyopathy, data on procedure-related major adverse events (MAE) in this population is lacking. were females.
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] Circulation 2007 2. Khan et al.
Image courtesy of Takenobu Shimada, Osaka Metropolitan University (CC BY 4.0, [link] mtaschetta-millane Mon, 07/29/2024 - 09:09 July 29, 2024 — When it comes to treating cardiacarrest, acting quickly can mean the difference between life and death. Cardiacarrest can lead to death within minutes. for both groups.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. Circulation [Internet] 2017;135(16):1481–9. Circulation. She was defibrillated and resuscitated.
Circulation, Ahead of Print. Out-of-hospital cardiacarrest is a leading cause of death, accounting for ≈50% of all cardiovascular deaths. The cardiac catheterization laboratory plays an important role in the coordinated Chain of Survival for patients with out-of-hospital cardiacarrest.
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. A reliable study would keep track of all patients with shockable arrest and analyze the ones who were not enrolled to see their outcomes. This is FAR LESS than all other studies of shockable arrest. 5% vs. 58%!!
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content