This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
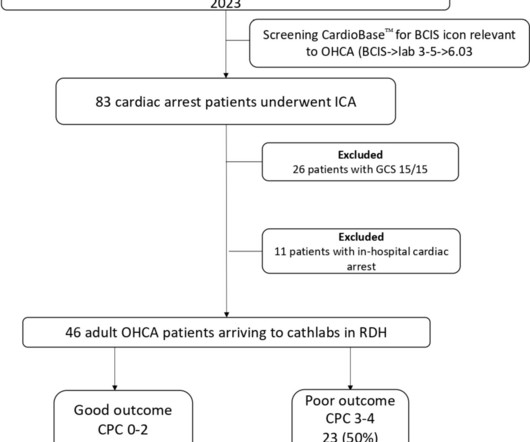
Introduction and objectives Decision-making regarding prognosticating out-of-hospitalcardiacarrest (OHCA) remains challenging at the front door. The study aims to validate the MIRACLE2 score in a district general hospital (DGH). Patients with a Glasgow Coma Scale of 15/15 after ROSC were excluded.
This randomized trial showed no significant difference in return of spontaneous circulation between initial intraosseous and intravenous vascular access in adults with out-of-hospitalcardiacarrest.
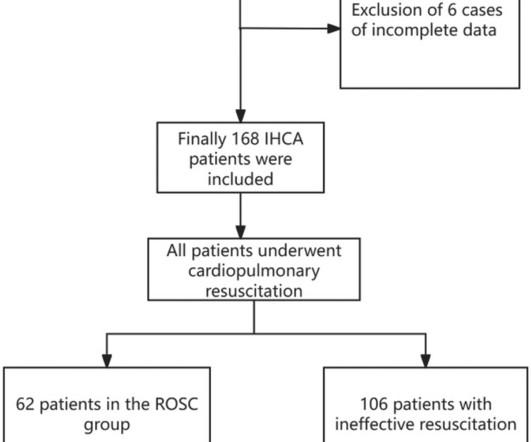
BackgroundIn-hospitalcardiacarrest (IHCA) refers to the occurrence of cardiacarrest in hospitalized patients requiring chest compressions and/or defibrillation, with only about one-third of patients achieving return of spontaneous circulation (ROSC) after cardiopulmonary resuscitation.
Circulation, Ahead of Print. People who experience out-of-hospitalcardiacarrest often require care at a regional center for continued treatment after resuscitation, but many do not initially present to the hospital where they will be admitted.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. AN evaluation of efficacy amonGst cOmpression only and standard CPR) trial is designed to evaluate whether compression-only cardiopulmonary resuscitation (CPR) by trained laypersons is noninferior to standard CPR in adult out-of-hospitalcardiacarrest.
In a prospective, multicentre, parallel, randomised clinical trial titled ARREST, researchers aimed to evaluate the effectiveness of expedited transfer to a cardiacarrest center compared to standard care following out-of-hospitalcardiacarrest. The ARREST study is the first randomized trial of its kind.
BackgroundOutofhospital cardiacarrest (OHCA) with initial shockable rhythm generally has a favorable prognosis. However, the prognosis worsens when this rhythm transitions to nonshockable rhythm on hospital arrival. The primary outcome was rhythm conversion to nonshockable on hospital arrival. On hospital arrival, 27.9%
The impact of chest compression (CC) pause duration on survival outcomes in pediatric in-hospitalcardiacarrests remains unclear, despite the American Heart Association’s recommendation to limit pauses to less than 10 seconds for children without solid evidence. Circulation 2024; 149: 1493-1500.
Circulation, Ahead of Print. Every 10 years, the American Heart Association (AHA) Emergency Cardiovascular Care Committee establishes goals to improve survival from cardiacarrest.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. Background:Prompt initiation of bystander cardiopulmonary resuscitation (CPR) is critical to survival for out-of-hospitalcardiacarrest (OHCA). Results:Of 78 048 patients with a witnessed OHCA treated with bystander CPR, the mean age was 63.5±15.7
Introduction The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (ECPR) in selected patients after out-of-hospitalcardiacarrest (OHCA) is an established method if return of spontaneous circulation cannot be achieved.
Circulation, Volume 150, Issue Suppl_1 , Page ASu505-ASu505, November 12, 2024. The targeted Automated External Defibrillator (AED) program in the Sao Paulo Metro has yielded promising results in improving survival rates for individuals experiencing out-of-hospitalcardiacarrest (OHCA) due to ventricular arrhythmias.
Circulation, Ahead of Print. BACKGROUND:In patients with out-of-hospitalcardiacarrest who present with an initial shockable rhythm, a longer delay to the first shock decreases the probability of survival, often attributed to cerebral damage. The mechanisms of this decreased survival have not yet been elucidated.
Does hospital median cardiopulmonary resuscitation (CPR) duration in patients without return of circulation (ROC) predict survival among hospitalized children?
Circulation, Volume 150, Issue Suppl_1 , Page A4141869-A4141869, November 12, 2024. Introduction:Over 290,000 in-hospitalcardiacarrests occur annually in the United States. Survival is about 25% with significant variation across the country.
BackgroundAlthough they are fastgrowing populations in the United States, little is known about survival outcomes of Hispanic and Asian patients after inhospital cardiac arrest.Methods and ResultsIn Get With The GuidelinesResuscitation, we identified Asian, Hispanic, and White adults with inhospital cardiacarrest during 2005 to 2023.
BackgroundDespite the wellknown importance of witnessed arrest and bystander cardiopulmonary resuscitation (CPR) for outofhospital cardiacarrest outcomes, previous studies have shown significant statistical inconsistencies. The outcome measure was prehospital return of spontaneous circulation (ROSC).
Although PAD can substantially increase the survival of cardiacarrest, PAD use remains low. The primary outcomes were the rate of bystander PAD use, sustained return of spontaneous circulation, survival to discharge, and favorable neurological outcomes. Journal of the American Heart Association, Ahead of Print.
Circulation, Volume 150, Issue Suppl_1 , Page ASu507-ASu507, November 12, 2024. Background:Most out-of-hospitalcardiacarrest (OHCA) patients who are initially treated with an automated external defibrillator (AED) and present in a non-shockable rhythm never receive a shock.
Circulation, Volume 150, Issue Suppl_1 , Page ASa505-ASa505, November 12, 2024. Moreover, the relationship between rSO2 and EtCO2 levels and ROSC was determined, as well as the influence of adrenaline and NaHCO3 supply on rSO2 values.Methods:A prospective observational study was performed at the University Hospital in Krakow (Poland).
Circulation, Volume 150, Issue Suppl_1 , Page ASu1202-ASu1202, November 12, 2024. C and hypothermia at 33°C had similar outcomes in out-of-hospital post cardiacarrest patients. Primary outcome was favorable neurological outcomes (cerebral performance categories of 1 or 2) at hospital discharge. 2018;22:226).
Circulation, Volume 150, Issue Suppl_1 , Page A4137905-A4137905, November 12, 2024. Background:In out-of-hospitalcardiacarrest (OHCA) patients with an initial shockable rhythm, epinephrine increases the likelihood of return of spontaneous circulation (ROSC), but its effect on neurological outcome remains uncertain.
Circulation, Volume 150, Issue Suppl_1 , Page A4137065-A4137065, November 12, 2024. Introduction:Out-of-hospitalcardiacarrest (OHCA) remains a significant public health challenge, with conventional cardiopulmonary resuscitation (CPR) often yielding limited success. to 7.30, I2: 47%) compared to conventional CPR.
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:There is no specific treatment for sudden cardiacarrest (SCA) manifesting as pulseless electric activity (PEA) and survival rates are low; unlike ventricular fibrillation (VF), which is treatable by defibrillation.
Circulation, Volume 150, Issue Suppl_1 , Page A4147424-A4147424, November 12, 2024. Table 1)Conclusions:The RA-AMC cohort are about 4 times more likely to require mechanical circulatory support during hospitalization for acute myocarditis, while IBD-AMC are less likely to have AHF.
Circulation, Volume 150, Issue Suppl_1 , Page A4118341-A4118341, November 12, 2024. Background:Opioid use has increased significantly in the past few decades, impacting cardiac and non-cardiac patients. Multivariate logistic and linear regression analyses were performed, adjusting for multiple patient and hospital confounders.
Circulation: Cardiovascular Interventions, Volume 18, Issue 1 , Page e014499, January 1, 2025. The primary outcome was a composite of 30-day mortality, resuscitated cardiacarrest, hemodynamic instability, and 90-day readmission. days;P=0.01) and hospital length of stay (5.0 days;P=0.046).
Circulation, Volume 150, Issue Suppl_1 , Page A4113864-A4113864, November 12, 2024. Background:Heart failure (HF) is one of the leading causes of hospitalizations in the States. Results:We included 4,454,273 weighted hospitalizations due to HF for which 380,446 patients (8.5%) had a concurrent diagnosis of hyperkalemia.
Circulation, Volume 150, Issue Suppl_1 , Page A4146863-A4146863, November 12, 2024. Data was obtained from the Hospital Corporation of America (HCA) enterprise-wide database from January 2020 to September 2023 using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM).
Circulation: Heart Failure, Ahead of Print. A secondary analysis evaluated outcomes for severe HF hospitalizations (cardiogenic shock, cardiacarrest, and mechanical ventilation). of centers), 525 037 (18.3%) were admissions to ATCs (5.5% of centers), and 15 541 (0.5%) were transferred to ATCs.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. Admissions to CICUs with the highest tertile of CCRx utilization had a greater burden of comorbidities, had more diagnoses of ST–elevation myocardial infarction, cardiacarrest, or cardiogenic shock, and had higher Sequential Organ Failure Assessment scores.
Circulation, Volume 150, Issue Suppl_1 , Page ASa404-ASa404, November 12, 2024. The four main metrics include time to shock (TTS), time to epinephrine administration, confirmation of airway (COA), and arrest monitored/witnessed. Goals:The NPD department reviewed GWTG-R data and survival to discharge at two hospitals.
But the lack of traditional Sgarbossa criteria is not reassuring enough for such high pretest probability (elderly patient with chest pain, out of hospitalcardiacarrest and LBBB), and the Modified Sgarbossa Criteria confirms Occlusion MI in this case. The patient still had chest pain and a third ECG was performed.
Hospital admission had been recommended, but she left that ED against medical advice. If cardiacarrest from hypokalemia is imminent (i.e., mEq of K pushed fast and circulated theoretically would raise serum K immediately by 1.0 There is some ST depression and peaked T-waves. mEq/L and a creatinine 1.5 mEq/L, from 1.9
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] Circulation 2007 2. Khan et al.
Getty Images milla1cf Fri, 06/14/2024 - 19:30 June 14, 2024 — Until now, known risk factors for cardiacarrest have been limited to cardiovascular conditions such as hypertension and high cholesterol. The findings appear in the journal Circulation. Upward of 400,000 people suffer a cardiacarrest every year in the U.S.,”
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content