This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A new observational study suggests the position in which responders initially place the two defibrillator pads on the body may make a significant difference in returning spontaneous blood circulation after shock from a defibrillator.
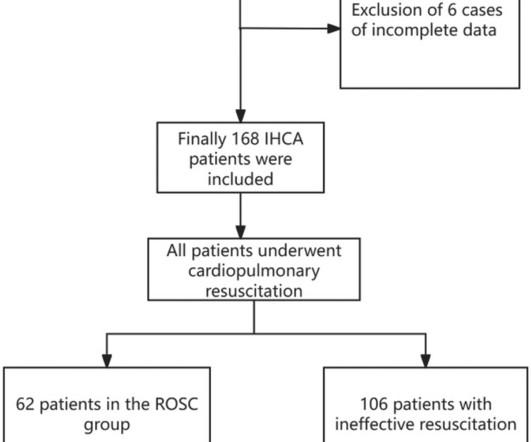
BackgroundIn-hospital cardiacarrest (IHCA) refers to the occurrence of cardiacarrest in hospitalized patients requiring chest compressions and/or defibrillation, with only about one-third of patients achieving return of spontaneous circulation (ROSC) after cardiopulmonary resuscitation.
Circulation, Volume 150, Issue Suppl_1 , Page ASu505-ASu505, November 12, 2024. The targeted Automated External Defibrillator (AED) program in the Sao Paulo Metro has yielded promising results in improving survival rates for individuals experiencing out-of-hospital cardiacarrest (OHCA) due to ventricular arrhythmias.
Circulation, Ahead of Print. Every 10 years, the American Heart Association (AHA) Emergency Cardiovascular Care Committee establishes goals to improve survival from cardiacarrest.
Circulation, Ahead of Print. BACKGROUND:In patients with out-of-hospital cardiacarrest who present with an initial shockable rhythm, a longer delay to the first shock decreases the probability of survival, often attributed to cerebral damage. This may explain the worse outcomes in patients with a long delay to defibrillation.
BackgroundPublic access defibrillation (PAD) programs have been implemented globally over the past decade. Although PAD can substantially increase the survival of cardiacarrest, PAD use remains low. Compared with the before‐run‐in group, the rate of successful automated external defibrillator acquisition was 13.5%
Circulation, Volume 150, Issue Suppl_1 , Page ASu507-ASu507, November 12, 2024. Background:Most out-of-hospital cardiacarrest (OHCA) patients who are initially treated with an automated external defibrillator (AED) and present in a non-shockable rhythm never receive a shock.
BackgroundDespite the wellknown importance of witnessed arrest and bystander cardiopulmonary resuscitation (CPR) for outofhospital cardiacarrest outcomes, previous studies have shown significant statistical inconsistencies. The outcome measure was prehospital return of spontaneous circulation (ROSC).
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
Circulation, Volume 150, Issue Suppl_1 , Page ASu404-ASu404, November 12, 2024. Background:Out-of-hospital cardiacarrest (OHCA) cause significant patient morbidity and mortality. Two-member teams established two defibrillators ready for rhythm analysis.
Although one may have all kinds of ischemic findings as a result of cardiacarrest (rather than cause of cardiacarrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think?
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:There is no specific treatment for sudden cardiacarrest (SCA) manifesting as pulseless electric activity (PEA) and survival rates are low; unlike ventricular fibrillation (VF), which is treatable by defibrillation.
Circulation, Volume 150, Issue Suppl_1 , Page A4137905-A4137905, November 12, 2024. Background:In out-of-hospital cardiacarrest (OHCA) patients with an initial shockable rhythm, epinephrine increases the likelihood of return of spontaneous circulation (ROSC), but its effect on neurological outcome remains uncertain.
Circulation, Volume 148, Issue 24 , Page e187-e280, December 12, 2023. The International Liaison Committee on Resuscitation engages in a continuous review of new, peer-reviewed, published cardiopulmonary resuscitation and first aid science.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. She was successfully revived after several rounds of ACLS including defibrillation and amiodarone.
If cardiacarrest from hypokalemia is imminent (i.e., Here is another post on hypoK: Patient with severe DKA, look at the ECG In this post, I discussed another patient I took care of : Prehospital CardiacArrest due to Hypokalemia I recently had a case of prehospital cardiacarrest that turned out to be due to hypokalemia.
Photo by Cedars-Sinai milla1cf Fri, 03/01/2024 - 08:25 March 1, 2024 — Two new studies by Cedars-Sinai investigators support using artificial intelligence (AI) to predict sudden cardiacarrest-a health emergency that in 90% of cases leads to death within minutes.
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. Coronary Angiography after CardiacArrest without ST-Segment Elevation. What percent of shockable arrests without STE have an OMI? These studies did not address OMI ECG findings!!! 5% vs. 58%!!
She was defibrillated and resuscitated. It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. Circulation [Internet] 2017;135(16):1481–9. Circulation.
Implantable Cardioverter-Defibrillator (ICD) to help manage dangerous heart rhythms. Regular physical activity can strengthen the heart and improve circulation. CardiacArrest or Sudden Death: Cardiomegaly increases the risk of life-threatening arrhythmias, which can cause sudden cardiacarrest.
She was never seen to be in ventricular fibrillation and was never defibrillated. What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. Circulation 122:Abstract 101.
Circulation, Volume 150, Issue Suppl_1 , Page A4139677-A4139677, November 12, 2024. Background:Epicardial patch defibrillators (EPDs) were commonly implanted in the 1990s for secondary prevention of sudden cardiac death. She experienced massive hemoptysis, leading to respiratory and cardiacarrest, but was resuscitated.
At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. If cardiacarrest from hypokalemia is imminent (i.e., mEq of K pushed fast and circulated theoretically would raise serum K immediately by 1.0
He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. Some episodes of PMVT would terminate spontaneously — but on many occasions, the PMVT degenerated to VFib, requiring defibrillation.
Circulation, Ahead of Print. The primary end point was AEs, defined as sudden cardiac death, sudden cardiacarrest, appropriate implantable cardioverter defibrillator shock, and arrhythmic syncope. mg/kg per day [interquartile range, 1.7–3.1]) 3.1]) were included. mg/kg per day [interquartile range, 1.7–3.1])
CASTLE-AF randomized 363 patients with atrial fibrillation and left ventricular ejection fraction of 35% or less, NYHA class II-IV heart failure and having an implanted defibrillator to either catheter ablation or medical therapy with rate or rhythm control [5]. Circulation. Circulation. N Engl J Med. doi: 10.1056/NEJMoa0708789.
Circulation, Ahead of Print. BACKGROUND:Declining cardiovascular mortality rates have been well-documented, yet temporal trends of sudden cardiac death (SCD) in young individuals remain unclear. to 28%, mainly because of increased bystander cardiopulmonary resuscitation and defibrillation rates.
Circulation, 117, 1890–1893. [3]: In addition to a spontaneous or induced Brugada-1 ECG pattern, criteria for B rugada S yndrome require one or more of the following: History of cardiacarrest, of polymorphoic VT, or of non-vagal syncope — positive family history of sudden death at an early age — a similar ECG in close relatives.
Getty Images milla1cf Tue, 01/30/2024 - 19:57 January 30, 2024 — Only 10% of people who experience a cardiacarrest survive. [1] Currently, 90% of people who experience cardiacarrest outside of a hospital die, in part because they do not receive CPR more than half of the time. [2]
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:Sudden cardiac death is the most common cause of death in childhood hypertrophic cardiomyopathy (HCM). Recently, 2 risk scores have been developed to estimate the 5-year risk of sudden cardiac death. males), with a mean follow-up of 8.65.5
We rapidly defibrillated her, and with return of normal sinus rhythm. Several minutes later the patient developed V-fib again > 200J defibrillation with return to NSR. Rapid sequence intubation was performed for airway protection in setting of recurrent V-fib and defibrillations. Chest X-ray also showed pulmonary edema.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content