This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Circulation, Ahead of Print. The criticalcare management of patients after cardiacarrest is burdened by a lack of high-quality clinical studies and the resultant lack of high-certainty evidence. Criticalcare management is crucial in patients after cardiacarrest and affects outcome.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. Admissions to CICUs with the highest tertile of CCRx utilization had a greater burden of comorbidities, had more diagnoses of ST–elevation myocardial infarction, cardiacarrest, or cardiogenic shock, and had higher Sequential Organ Failure Assessment scores.
They shocked him twice before return of spontaneous circulation. Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing criticalcare. Frick's presentation in today's case is its simplicity in conveying a critically important finding affecting the outcome of this patient.
If cardiacarrest from hypokalemia is imminent (i.e., mEq of K pushed fast and circulated theoretically would raise serum K immediately by 1.0 As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 Crit Care Med. Setting: Multidisciplinary criticalcare unit.
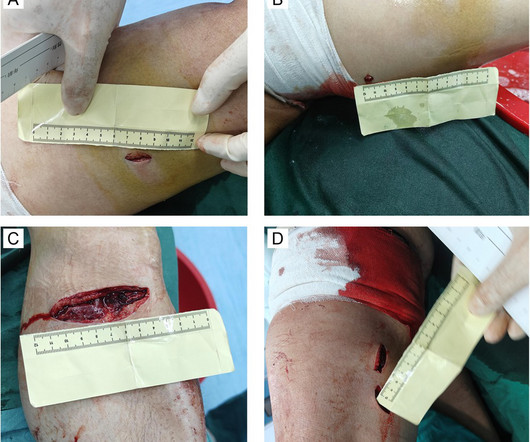
BackgroundTraumatic cardiacarrest (TCA) poses significant challenges in resuscitation, with extremely high mortality rates, making it a critical issue in emergency and criticalcare medicine. The patient experienced cardiacarrest upon admission to a local hospital.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content