This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. In this case, the EMS provider was routed to the urgent care facility.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. Just as important is pretest probability: did the patient report chestpain prior to collapse?
A 20-something male drank heavily of ethanol and used cocaine, then was involved in a stressful verbal altercation, at which time he developed chestpain. 911 was called and the medics recorded this ECG (unfortunately, leads V4-V6 are missing) Due to marked ST Elevation, the computer read was STEMI What do you think?
A small proportion of patients with STEMI treated via primary PCI experienced late ventricular tachycardia (VT) or ventricular fibrillation (VF), occurring one or more days following the procedure, but late VT or VF with cardiacarrest occurred rarely, especially among patients with uncomplicated STEMI, according to a study published in JAMA Network (..)
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. These studies did not address OMI ECG findings!!!
A woman in her 50s with dyspnea and bradycardia A patient with cardiacarrest, ROSC, and right bundle branch block (RBBB). HyperKalemia with CardiacArrest. Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia What will you do for this altered and bradycardic patient? What is it?
This 80 year old with a history of CABG had a cardiacarrest. He did not state he had chestpain, but, then again, he couldn't remember anything. This is as clear a STEMI as you can get. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome!
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chestpain and SOB. She had been sitting doing work when she experienced "waves of chest tightness". Sats were 88%.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. EMS recorded the following ECG: What do you see?
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. His initial troponin T was 15 ng/L (only two hours since pain onset). He stated it was similar to prior heart attacks.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chestpain with paresthesias of the left arm. A repeat ECG was recorded with pain 2/10: Not much change.
There is no way to tell the difference between GI etiology of chestpain and MI. Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chestpain are nearly diagnostic of ischemia. Could this have been avoided? Lesson : 1.
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. Potassium was normal. Take home 1.
He complained of severe chestpain and was extremely agitated, so much so that he was throwing chairs in triage. Technically, the STE meets STEMI criteria because there is greater than 2.5 These kinds of cases were excluded from the study as obvious anterior STEMI. His chestpain resolved. What do you think?
The patient presented with chestpain. If it is STEMI, it would have to be RBBB with STEMI. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. This ECG was sent from South Asia.
The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiacarrest. Anterolateral STEMI. The formula results in 23.43, just above the 23.4 He was defibrillated. Here is his post resuscitation ECG: Now the diagnosis is obvious.
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI. Smith's ECG Blog ).
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. He had multiple cardiacarrests with ROSC regained each time. Submitted by a Med Student, with Great Commentary on Bias!
A late middle-aged man presented with one hour of chestpain. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? If cardiacarrest from hypokalemia is imminent (i.e., to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5
He did not have chestpain. Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest. Is it STEMI? Chestpain in high risk patient. Here is his triage ECG: What do you think? What does the ECG show? Also see the bizarre Bigeminy.
link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! We at HCMC have 30 walk-in STEMIs per year; the rest come by ambulance. Am J Emerg Med 36(10):1771-1774.
A 50-something presented with epigastric and chestpain. Saddleback ST Elevation is almost never STEMI 2. Here are other cases of saddleback STE: Is this Saddleback a STEMI?? Here is his ECG: What do you think? QTc 388 ms. The patient was diagnosed with reflux Learning Points : 1. wave in V1?? wave in V1??
There was no chestpain. The cath lab was activated for STEMI. Unfortunately, the patient had a cardiacarrest on arrival to the cath lab, before return of the potassium. So, in retrospect, the first patient probably did not have STEMI at all. Hyperkalemia can result in ST elevation that imitates STEMI 3.
He was at the gym when he had the onset of chestpain. RBBB in acute STEMI has a very high mortality. Were it not for this prehospital ECG and the cardiacarrest, the diagnosis may have been significantly delayed. This patient is 38 years old with hyperlipidemia. There is a wide S-wave in V6.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). Having looked for negative U waves in patients with chestpain over a period of decades — I'll emphasize that this is not a common finding.
Apparently he denied chestpain. The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." About two hours after admission, he suffered a cardiacarrest (whether it was VF/VT or PEA is not available) and expired. Canto et al.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology.
Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. The case was reviewed by all parties, and it was stated correctly that the ECG does not meet the STEMI criteria.
It turns out that this was a 27 yo African American male who presented with pressure-like (non-pleuritic) chestpain and dyspnea. Here is a case of a 45 year old with chestpain: There is ST elevation in inferior leads only, with no reciprocal ST depression in aVL. Would you be certain that it is not STEMI?
He has done a lot of great work on cardiacarrest, including as co-author of our study on esmolol in refractory cardiacarrest, and much more with Keith Lurie. A 40-something woman was in a remote alpine location when she complained of crushing chestpain. See his Google Scholar profile here.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. Case 3 : Male in 30's with chestpain, cough, and fever. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think?
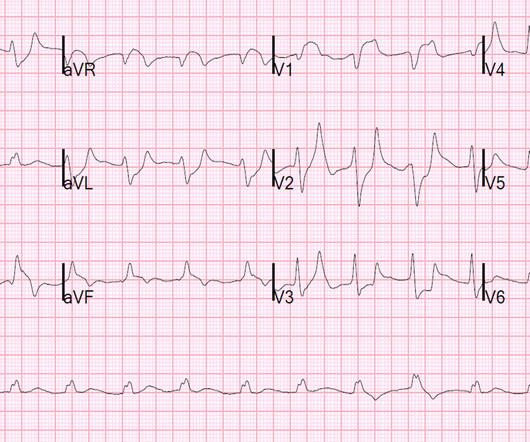
This middle aged patient presented with chestpain: What do you think? There is VERY low voltage. There is some ST Elevation, but it is MINIMAL. But look how small the QRS is!! Let's stretch out the QRS vertically so it is not so tiny: On upper left is the original.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. What is it?
This pattern is essentially always accompanied by cardiogenic shock and high rates of VT/VF arrest, etc. Code STEMI was activated. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery. Plus recommendations from a 5-member panel on cardiacarrest.
Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), In Septal STEMI , transmural ischemia of the septum is recorded by the overlying lead V1 as ST Elevation. Lead III is also on the right and might manifest ST Elevation in Septal STEMI. with ADDED STE in III?
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. Patients on dialysis often do not have chestpain in the setting of acute MI. Why is this?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content