This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. In this case, the EMS provider was routed to the urgent care facility.
The chestpain quickly subsided. Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. After about 90 seconds of chest compressions she awoke. Calcium level was normal.
The ECG shows severe ischemia, possibly posterior OMI. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another.
There is no way to tell the difference between GI etiology of chestpain and MI. Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chestpain are nearly diagnostic of ischemia. Could this have been avoided? Lesson : 1.
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. The ECG does not show any definite signs of ischemia. The below ECG was recorded.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chestpain with paresthesias of the left arm. A repeat ECG was recorded with pain 2/10: Not much change.
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiacarrest. Ischemia comes and goes. He was defibrillated. Anterolateral STEMI.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. Ischemic ST depression includes posterior OMI and subendocardial ischemia.
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. Potassium was normal. Cardiology did not think it was "STEMI", but repeated the troponin. Take home 1.
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. A recent similar case: A 40-something with chestpain. Is this inferior MI?
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain. Vitals were HR 58 BP 167/70 R20 sat 96%.
An ECG was recorded during pain: What do you think? This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. These suggest inferior OMI with possible RV involvement. with ADDED STE in III?
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history? J Electrocardiol 2013;46:240-8 2.
He has done a lot of great work on cardiacarrest, including as co-author of our study on esmolol in refractory cardiacarrest, and much more with Keith Lurie. A 40-something woman was in a remote alpine location when she complained of crushing chestpain. See his Google Scholar profile here. It was not.
Case A 47 year old male called 911 for severe chestpain. He had a previous MI with cardiacarrest 2 years prior. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. Data from stress testing proves that the ST depression of ischemia does not localize.
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. It should be known that each category can easily manifest the generic subendocardial ischemia pattern.
No chestpain. Figure-1: The initial ECG in today's case — obtained from an 86-year old man with presyncope, but no chestpain. ( The other main consideration — is to take another look at the 12-lead ECG, and assess this for recent ischemia or infarction. How would YOU interpret the ECG in Figure-1 ?
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
If a patient presents with chestpain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise. This, in turn, could produce platelet aggregation and vasospasm and result in an acute coronary syndrome." Clinical Context is everything !
This suggests ischemia of uncertain duration. Unfortunately, before this could be accomplished — the patient went into cardiacarrest. She was successfully resuscitated — with a post-arrest rhythm similar to that seen in Figure-1. Cardiac cath did not reveal significant coronary disease!
This is often quite challenging to recognize — but the finding of negative U waves in a patient with chestpain is highly suggestive of ischemia ! N OTE # 2 — On rare occasions, the U wave may be negative. Figure-2: Sequential development of ST-T wave changes with hypokalemia. Note increasing U wave amplitude ( See text ).
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
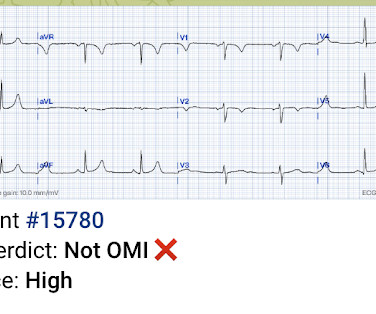
Case submitted by Magnus Nossen MD from Norway, written by Pendell Meyers A man in his 50s with no pertinent medical history suffered a witnessed cardiacarrest. 12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. She was noted to be tachycardic and her heart sounds were distant on physical exam.
This was interpreted by the treating clinicians as not showing any evidence of ischemia. However, he did not remember much from the day of the arrest. He did not remember whether he had experienced any chestpain. He was intubated in the field and sedated upon arrival at the hospital. He was admitted to cardiology.
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. CardiacArrest or Sudden Death: Cardiomegaly increases the risk of life-threatening arrhythmias, which can cause sudden cardiacarrest.
A 20-something male drank heavily of ethanol and used cocaine, then was involved in a stressful verbal altercation, at which time he developed chestpain. See this post and associated case reports: Cardiacarrest, severe acidosis, and a bizarre ECG The patient was admitted and ruled out for acute MI by serial troponins.
He did not have chestpain. A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." Chestpain in high risk patient. What does the ECG show?
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent!
The patient presented with chestpain. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada.
All of the patients presented with chestpain , and they are all in triage. Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. True Positive ECG#2 : Also sinus rhythm.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain? There is STE in aVR.
No chestpain. Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). Later on during the night of his admission he had a short episode of chestpain that resolved with sublingual nitroglycerin. His vitals were initially normal.
A late middle-aged man presented with one hour of chestpain. If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. If cardiacarrest from hypokalemia is imminent (i.e., Most recent echo showed EF of 60%.
If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause. CardiacarrestCardiacarrest is a medical emergency in which the heart stops pumping blood to the body.
Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher.
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). What is the Diagnosis in this 70-something with ChestPain?
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. There is no definite evidence of acute ischemia. (ie, The below ECG was recorded.
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. He could not be resuscitated.
Case 3 : Male in 30's with chestpain, cough, and fever. Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was Was the ST elevation due to transient demand ischemia, or is it false positive? What do you think? He has clinical pneumonia. Called 911. Does he need a stress test? --Is
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. TOP Initial ECG of this 60-year old man with a history of prior MI, who presented with new-onset chestpain.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content