This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Photo by Cedars-Sinai milla1cf Fri, 03/01/2024 - 08:25 March 1, 2024 — Two new studies by Cedars-Sinai investigators support using artificial intelligence (AI) to predict sudden cardiacarrest-a health emergency that in 90% of cases leads to death within minutes.
She is healthy with no known cardiac disease. A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. The chestpain quickly subsided. What do you think?
He was intubated in the field and sedated upon arrival at the hospital. However, he did not remember much from the day of the arrest. He did not remember whether he had experienced any chestpain. At his family's request, he was transferred to a hospital closer to his home to continue care.
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. Just as important is pretest probability: did the patient report chestpain prior to collapse?
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chestpain and SOB. Probably because of a high troponin with chestpain.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. The patient had a protracted hospitalization and did not survive.
Introduction Sudden cardiacarrest is a major cause of morbidity and mortality worldwide and remains a major public health problem for which better non-invasive prediction tools are needed. The individual relationship between fatal arrhythmias and cardiac function abnormalities in predicting cardiac death risk has rarely been explored.
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. Coronary Angiography after CardiacArrest without ST-Segment Elevation. N Engl J Med [Internet] 2019;Available from: [link] Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. He had multiple cardiacarrests with ROSC regained each time. He was prescribed apixaban. What is the Diagnosis?
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation.
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. Potassium was normal. Cardiology did not think it was "STEMI", but repeated the troponin. Take home 1.
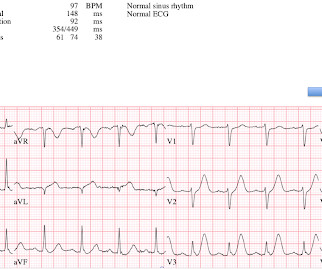
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
He did not have chestpain. The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest. Chestpain in high risk patient.
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. She felt nauseous and lightheaded with no neurologic deficits.
Written by Pendell Meyers We received a call from an outside hospital asking to transfer a "traumatic post arrest" patient. We were told that a young patient was brought in with altered mental status but complaining of right hip and/or leg pain after being found by his mother at the bottom of the stairs into the basement.
BACKGROUND:There is no specific treatment for sudden cardiacarrest (SCA) manifesting as pulseless electric activity (PEA) and survival rates are low; unlike ventricular fibrillation (VF), which is treatable by defibrillation. Circulation: Arrhythmia and Electrophysiology, Ahead of Print.
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. C ASE C onclusion: As noted above — the middle-aged man in today's case presented to the ED in cardiacarrest. In view of this history — How would YOU interpret the ECG in Figure-1 ?
In fact, most do not make it to the hospital alive, which explains why only a tiny percent of OMI are due to full LM occlusion. Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiacarrest, cardiogenic shock or impending shock.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
C harges and cost have no relation to each other in hospital billing. No, again, charges and cost have no relation to each other in hospital billing. We record ECGs in triage on every patient with chestpain, and some other indications, and this amounts to 8000 ECGs in triage each year, costing at most $200,000 (8000 x $20.00).
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain. Vitals were HR 58 BP 167/70 R20 sat 96%.
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. Here is his ECG on arrival: What do you think?
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The patient was extubated on Day-3 of the hospital stay. The below ECG was recorded.
A late middle-aged man presented with one hour of chestpain. If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 The mean serum potassium level was lower after resuscitation from cardiacarrest (3.6
Apparently he denied chestpain. About two hours after admission, he suffered a cardiacarrest (whether it was VF/VT or PEA is not available) and expired. JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain. Here is his first ED ECG: What do you see?
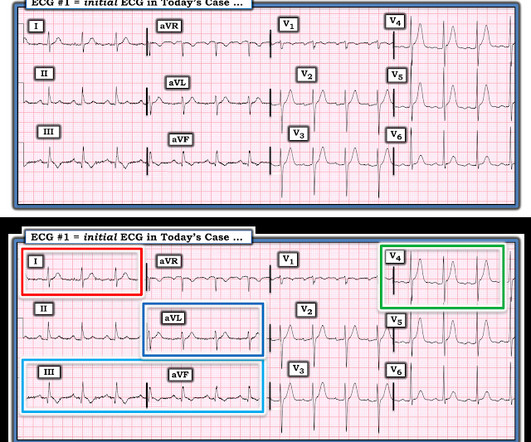
LEARNING Point: Maximal ST depression in leads V2-thru-V4 ( especially when the ST-T waves are shaped as they are in ECG #1 ) in a patient with new chestpain ( or sudden cardiacarrest, as in today’s case ) — is diagnostic of acute Posterior OMI until proven otherwise!
Other cases of LAD OMI with RBBB/LAFB: A man in his 40s who really needs you to understand his ECG CardiacArrest at the airport, with an easy but important ECG for everyone to recognize A woman in her 60s with 6 hours of chestpain, dyspnea, tachycardia, and hypoxemia Ventricular Fibrillation, ROSC after perfusion restored by ECMO, then ECG.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. Steve, what do you think of this ECG in this CardiacArrest Patient?" What is it?
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Unfortunately — the patient abruptly developed hypoxemia, followed by cardiacarrest with PEA. Apparently while waiting on the hospital floor for the decision regarding optimal aortic replacement — the patient took one of his sublingual NTG ( nitroglycerin ) tablets. He could not be resuscitated.
Case A 47 year old male called 911 for severe chestpain. He had a previous MI with cardiacarrest 2 years prior. A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chestpain with radiation to the anterior neck, with associated nausea.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography.
And she does not know that this is an overdose; she thinks it is a patient with chestpain!! This meets the Smith Modified Sgarbossa criteria, but the situation is wrong for diagnosing OMI!! By the way, the PM Cardio Bot Queen of Hearts says this is Not OMI with High Confidence. 3 hours later, this was recorded at a K of 2.8
My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. Unfortunately, before this could be accomplished — the patient went into cardiacarrest. Cardiac cath did not reveal significant coronary disease!
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. The formal diagnosis codes were populated to the chart by the primary hospitalization teams.
However, according to these diagnostic criteria (JACC 2011; 57(7):802), it is a Bazett corrected QT of less than 330-370, depending on other diagnostic criteria, including 1) h/o cardiacarrest, 2) sudden syncope, 3) family hx of sudden unexplained arrest at age less than 40, 4) family hx of SQTS. Some other points: 1.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? She was discharged after a short hospitalization with oncology and cardiology follow-up. She was noted to be tachycardic and her heart sounds were distant on physical exam. This patient is only pseudo-stable.
This patient had many complaints including chestpain. Comment by K EN G RAUER, MD ( 2/11 /2023 ): = Today’s case is from a patient with “many complaints”, including chestpain — and, an ECG that raised concern about acute anterior OMI. The computer called this Acute STEMI What do you think? The ioninzed calcium was 6.5
Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 Here is the history: 62 yo male w 2d of intermittent chestpain, now constant. Here is a more detailed history: Presented to the emergency department with chestpain. My response was: "It depends on the patient.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content