This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
If a patient presents with chestpain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise. CLICK HERE — for the ESC/ACC/AHA/WHF 2018 Consensus Document on the 4th Universal Definition of MI, in which these concepts are discussed and illustrated.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? This patient was reported to have distant heart sounds but was not hypotensive and did not have JVD according to documentation. She was noted to be tachycardic and her heart sounds were distant on physical exam.
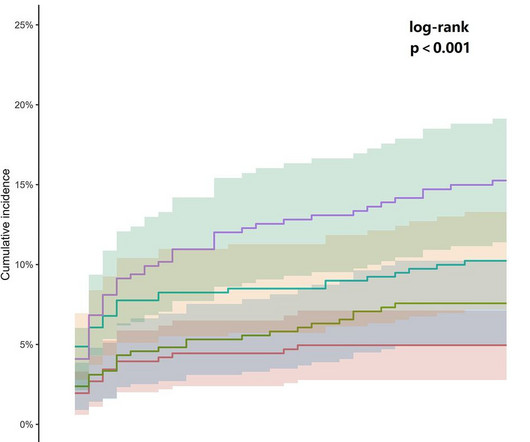
ObjectiveAlthough the association between admission glucose (AG) and major adverse cardiac events (MACE) is well-documented, its relationship with 30-day MACE in patients presenting with cardiacchestpain remains unclarified.
A late middle-aged man presented with one hour of chestpain. If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 The mean serum potassium level was lower after resuscitation from cardiacarrest (3.6
Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. In both tracings — an exceedingly fast PMVT is documented. The below ECG was recorded.
It was from a patient with chestpain: Note the obvious Brugada pattern. Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. The elevated troponin was attributed to either type 2 MI or to non-MI acute myocardial injury. There is no further workup at this time.
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. Further history later: This patient personally has no further high risk features (syncope / presyncope), but her mother had sudden cardiacarrest in sleep.
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." Unexplained cardiacarrest or documented VF/polymorphic VT: +3 3. Cardiacarrest.
He played a round of golf a week prior and felt an episode of chestpain during the round, which spontaneously resolved. On presentation, he reported no chestpain or shortness of breath. The patient should have immediately been sent for further cardiac evaluation at a PCI center based on this EKG.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content