This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. The ECG was also interpreted as normal by the primary care physician.
The chestpain quickly subsided. Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. After about 90 seconds of chest compressions she awoke. Calcium level was normal.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. They started CPR.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chestpain with paresthesias of the left arm. A repeat ECG was recorded with pain 2/10: Not much change.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
Patients may feel a fluttering in the chest, chestpain, shortness of breath and dizziness or lightheadedness as a result. If VT is not treated, it can lead to cardiacarrest, which is when the heart stops beating. In fact, VT is the most common cause of sudden cardiacarrest.
The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiacarrest. He was defibrillated. The formula results in 23.43, just above the 23.4 Here is his post resuscitation ECG: Now the diagnosis is obvious. Anterolateral STEMI.
A 56 yo f with h/o HTN and hypercholesterolemia called EMS from home after onset of L chestpain radiating to the left arm. She was defibrillated successfully from ventricular fibrillation and developed a perfusing rhythm. Before EMS arrived, she had "seizure activity" and became unresponsive. She was intubated.
A 60-something woman presented after a witnessed cardiacarrest. She was never defibrillated. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. A recent similar case: A 40-something with chestpain.
BACKGROUND:There is no specific treatment for sudden cardiacarrest (SCA) manifesting as pulseless electric activity (PEA) and survival rates are low; unlike ventricular fibrillation (VF), which is treatable by defibrillation. Circulation: Arrhythmia and Electrophysiology, Ahead of Print.
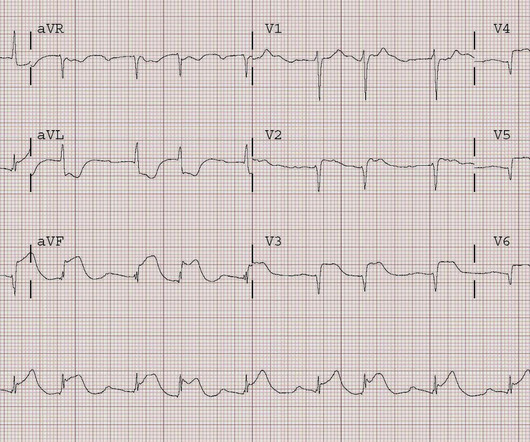
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. C ASE C onclusion: As noted above — the middle-aged man in today's case presented to the ED in cardiacarrest. A series of VFib episodes followed — each time with successful defibrillation.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. She was defibrillated and resuscitated.
When discussing heart health, heart attacks and cardiacarrest are two terms that are often mistaken for one another. Understanding the difference between heart attack and cardiacarrest can help in recognizing symptoms, seeking prompt medical care, and even saving lives. What is CardiacArrest?
I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right?
Case submitted by Magnus Nossen MD from Norway, written by Pendell Meyers A man in his 50s with no pertinent medical history suffered a witnessed cardiacarrest. 12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC.
Photo by Cedars-Sinai milla1cf Fri, 03/01/2024 - 08:25 March 1, 2024 — Two new studies by Cedars-Sinai investigators support using artificial intelligence (AI) to predict sudden cardiacarrest-a health emergency that in 90% of cases leads to death within minutes. It cannot be treated with a defibrillator and often leads to death.
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. Coronary Angiography after CardiacArrest without ST-Segment Elevation. Do not disregard the initial 12 lead ECG after out-of-hospital cardiacarrest: It predicts angiographic culprit despite metabolic abnormalities.
Implantable Cardioverter-Defibrillator (ICD) to help manage dangerous heart rhythms. CardiacArrest or Sudden Death: Cardiomegaly increases the risk of life-threatening arrhythmias, which can cause sudden cardiacarrest. Heart Transplant may be considered in severe cases where other treatments have failed.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. CPR was initiated immediately.
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardial infarction of any kind. Is it Brugada pattern?
Introduction Sudden cardiacarrest is a major cause of morbidity and mortality worldwide and remains a major public health problem for which better non-invasive prediction tools are needed. Primary preventive therapies, such as implantable cardioverter defibrillators, are not personalized and not predictive.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
He was at the gym when he had the onset of chestpain. Were it not for this prehospital ECG and the cardiacarrest, the diagnosis may have been significantly delayed. Had this happened, the artery may have re-occluded prior to angiography, with resultant recurrent cardiacarrest and/or shock and death.
A late middle-aged man presented with one hour of chestpain. At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. If cardiacarrest from hypokalemia is imminent (i.e., mEq/L, from 1.9
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. He required multiple defibrillations within a period of a few hours. What do you think?
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. In the ambulance during transport, the patient suddenly suffered VF arrest.
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. Although in the context of chestpain such ST depression would be all but diagnostic of posterior OMI, one should make no conclusions in such an unusual case.
It was from a patient with chestpain: Note the obvious Brugada pattern. The elevated troponin was attributed to either type 2 MI or to non-MI acute myocardial injury. There is no further workup at this time. Smith: Here is a case that was just texted to me today from a former resident. This patient ruled out for MI.
This patient had many complaints including chestpain. Comment by K EN G RAUER, MD ( 2/11 /2023 ): = Today’s case is from a patient with “many complaints”, including chestpain — and, an ECG that raised concern about acute anterior OMI. Treatment is by ICD ( implantable cardioverter defibrillator ).
A 65 yo woman had felt ill for 36 hours, had seen her MD but without undergoing a cardiac evaluation. After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. Exact rhythm during arrest is uncertain. She collapsed and 911 was called; she was found pulseless. These patients may survive.
Written by Pendell Meyers A man in his 60s presented with acute chestpain. He was sent back to the waiting room, where he suffered a VF arrest. Defibrillation was performed, and ROSC was achieved. Smith comment: The patient was lucky to have a cardiacarrest. Here is his triage ECG: What do you think?
Further history later: This patient personally has no further high risk features (syncope / presyncope), but her mother had sudden cardiacarrest in sleep. The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. We repeated the ECG: Brugada pattern is mostly resolved.
A middle-age woman with no previous cardiac history called 911 for chestpain. We rapidly defibrillated her, and with return of normal sinus rhythm. Several minutes later the patient developed V-fib again > 200J defibrillation with return to NSR. Chest X-ray also showed pulmonary edema. Potassium was 4.5
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content