This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Patient has an ICD, which is primarily placed in patients with cardiomyopathy.
The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Polymorphic ventricular tachycardia can be ischemic, catecholaminergic or related to QT prolongation. Cardiacarrest was called and advanced life support was undertaken for this patient. Without an MRI, it is impossible to know.
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiacarrest, defibrillated, diffuse ST depression and ST Elevation in aVR.
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. Bedside cardiac ultrasound showed moderately decreased LV function. See this post: How a pause can cause cardiacarrest 2. The plan: 1.
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? The patient was diagnosed with stress cardiomyopathy. The QTc then gradually shortened over the course of several days as is usual for stress cardiomyopathy.
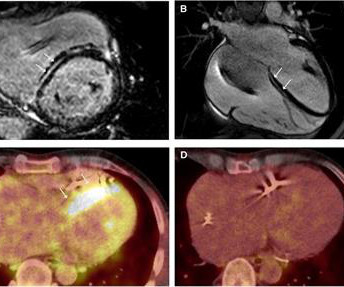
Cardiac sarcoidosis (CS), a rare condition characterized by non-caseating granulomas, can manifest with symptoms such as atrioventricular block and ventricular tachycardia (VT), as well as mimic inherited cardiomyopathies. A 48-year-old male presented with recurrent VT. Genetic testing identified a pathogenic mutation in PKP2.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. T wave alternans is a harbinger of cardiac instability and TdP. (3) No ischemic ST changes.
Although one may have all kinds of ischemic findings as a result of cardiacarrest (rather than cause of cardiacarrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think?
This sinus tachycardia ( at ~130/minute ) — is consistent with the patient’s worsening clinical condition, with development of cardiogenic shock. This list takes on new relevance given the ongoing Covid-19 pandemic — which predisposes to acute thrombotic events, stress cardiomyopathy ( Takotsubo ), infarction/ischemia and myocarditis.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. If a patient presents with chest pain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise.
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. CardiacarrestCardiacarrest is a medical emergency in which the heart stops pumping blood to the body. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiacarrest.
Video-based AI A profound learning approach is created with a video-based neural system that utilizes a current database of video formats to determine cardiac issues. The deep learning algorithm helps segment the left ventricle predicting cardiomyopathy and ejection fraction. AI recognizing cardiacarrests in emergency calls.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
Other than tachycardia, Other than slight tachycardia, vitals were within normal limits (including oxygen saturation). As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. The PR interval is normal.
NOTE: As discussed in detail in ECG Blog #108 — " A IVR" is an "enhanced" ventricular ectopic rhythm that occurs faster than the intrinsic ventricular escape rate ( which is typically between 20-40/minute ) — but slower than hemodynamically significant Ventricular Tachycardia ( ie, VT at rates >130-140/minute ).
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy. The final letter in the SLOWED mnemonic is " D " for "Dead" ( resulting from VT/VF or asystolic cardiacarrest ). Occurrence of “J Waves” in 12-Lead ECG as a Marker of Acute Ischemia and Their Cellular Basis.
There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. Resuscitation was begun with chest compressions, etc.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content