This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiacarrest, defibrillated, diffuse ST depression and ST Elevation in aVR.
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. What is the utility of a head CT in cardiacarrest?
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
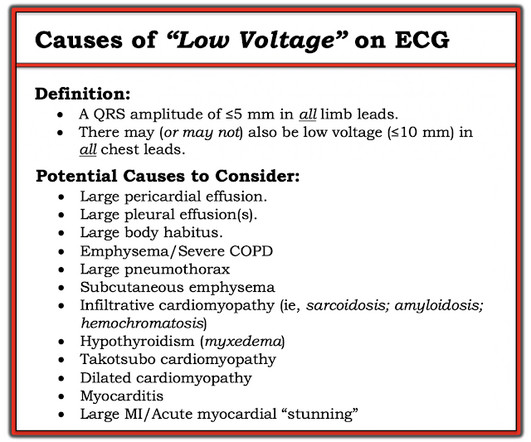
In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 But a look at Figure-2 reminds us of a long list of additional entities to consider!
This phenomenon has been associated with cardiacarrest; after cardiac surgery; post-cardioversion following a sustained tachyarrhythmia; with certain types of acute cerebrovascular events ( such as subarachnoid hemorrhage ) — and , in association with large acute MI , which could potentially be the clinical scenario in today's case!
As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." Canto et al.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy. The impact of ST-segment elevation on the prognosis of patients with Takotsubo cardiomyopathy. From Gue at al.
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
A 12-lead was recorded, showing "STEMI," but is unavailable. The patient was unconscious BEFORE the cardiacarrest, at the same time that she had strong pulses. Therefore, cardiacarrest is NOT the etiology of the coma. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content