This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The chestpain quickly subsided. Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. After about 90 seconds of chest compressions she awoke. The patient did well.
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. Just as important is pretest probability: did the patient report chestpain prior to collapse?
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
CardiomyopathyCardiomyopathy is a condition that affects the heart muscle, causing it to become enlarged, thick, or rigid. Excessive Alcohol or Drug Use Long-term abuse of alcohol or certain drugs can weaken the heart muscle, resulting in cardiomyopathy and eventually cardiomegaly.
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. She felt nauseous and lightheaded with no neurologic deficits.
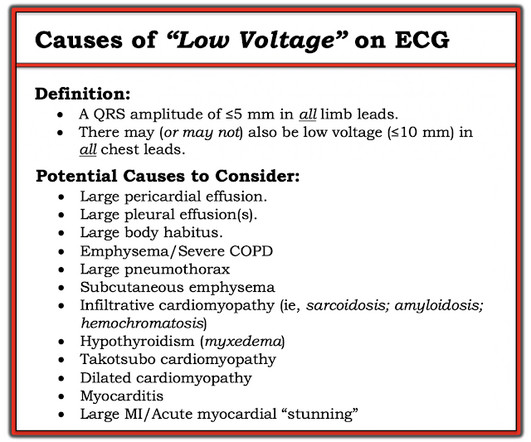
This middle aged patient presented with chestpain: What do you think? There is VERY low voltage. There is some ST Elevation, but it is MINIMAL. But look how small the QRS is!! Let's stretch out the QRS vertically so it is not so tiny: On upper left is the original.
If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause. CardiacarrestCardiacarrest is a medical emergency in which the heart stops pumping blood to the body.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Apparently he denied chestpain. As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain.
No chestpain. Figure-1: The initial ECG in today's case — obtained from an 86-year old man with presyncope, but no chestpain. ( It may also occur in patients with underlying coronary disease, cardiomyopathy, and/or with digoxin toxicity. Th e patient was hemodynamically stable in association with this rhythm.
If a patient presents with chestpain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise. Thus, there is a wall motion abnormality in the distribution of the LAD (not global apical dyskinesis, as in takostubo). Clinical Context is everything !
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? The most important clinical entity associated with motion alternans is large pericardial effusion — though motion alternans has also been observed in some cases of hypertrophic cardiomyopathy.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content