This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 55-year-old man had an out-of-hospitalcardiacarrest. An evaluation showed 2-mm ST-segment elevations in the inferior leads on electrocardiography, cardiogenicshock, and a new systolic murmur. A diagnosis was made.
A 20-something presented after a huge verapamil overdose in cardiogenicshock. Today's patient is a young male who presented in cardiogenicshock following a massive verapamil overdose. He had been seen at an outside institution and been given 6 g calcium gluconate, KCl, and a norepinephrine drip. The initial K was 3.0
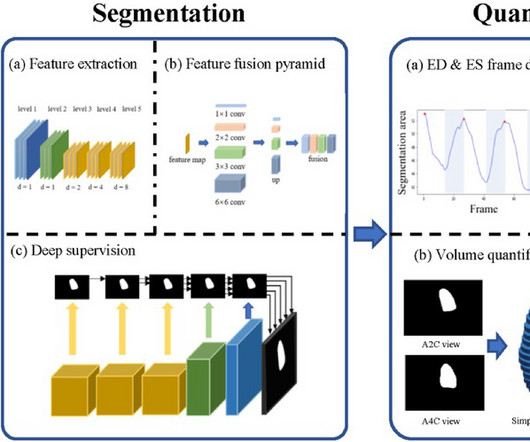
BackgroundPercutaneous extracorporeal membrane oxygenation (ECMO) is administered to pediatric patients with cardiogenicshock or cardiacarrest. The traditional method uses focal echocardiography to complete the left ventricular measurement.
Introduction The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (ECPR) in selected patients after out-of-hospitalcardiacarrest (OHCA) is an established method if return of spontaneous circulation cannot be achieved.
BackgroundAcute myocardial infarction complicated by cardiogenicshock (AMI‐CS) is associated with significant morbidity and mortality. The primary end point was in‐hospital mortality. Survival rates to hospital discharge were high. A total of 406 patients were enrolled at 80 sites between 2016 and 2020.
BackgroundCardiogenic shock complicating acute myocardial infarction is associated with a high mortality rate. Cardiogenicshock after outofhospital cardiacarrest (OHCA) can be due to transient myocardial stunning but also reflect the increasing severity of ongoing heart failure.
Impella and venoarterial extracorporeal membrane oxygenation (VA-ECMO) in patients with acute myocardial infarction-related cardiogenicshock (AMICS). Impella patients were older (34% vs. 13% >75 years, p < 0.001) and less frequently presented after an out-of-hospitalcardiacarrest (18% vs. 40%, p < 0.001).
Introduction The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (eCPR) has emerged as a treatment option for selected patients who are experiencing refractory cardiacarrest (CA).
Multivariate logistic and linear regression analyses were performed, adjusting for multiple patient and hospital confounders. There was a non-significant increased risk of cardiogenicshock (aOR 1.14, 95% CI 0.87 - 1.5, p=0.35) and cardiacarrest (aOR 1.05, 95% CI 0.8 - 1.36, p=0.74) in patients on chronic opioids.
Secondary outcomes included in-hospital and 30-day events. SMuRF-less patients were more likely to present with cardiacarrest (6.6% vs 50.8%, p<0.001) and were more likely to experience postprocedural cardiogenicshock (4.5% Methods We analysed data from the Melbourne Interventional Group PCI Registry.
A secondary analysis evaluated outcomes for severe HF hospitalizations (cardiogenicshock, cardiacarrest, and mechanical ventilation). Centers performing at least 1 heart transplant or left ventricular assist device were classified as ATCs. of centers), 525 037 (18.3%) were admissions to ATCs (5.5%
This analysis included 17 843 admissions across 34 sites and compared interhospital tertiles of CCRx (eg, mechanical ventilation, mechanical circulatory support, continuous renal replacement therapy) utilization and its adjusted association with in-hospital survival using logistic regression.
But the lack of traditional Sgarbossa criteria is not reassuring enough for such high pretest probability (elderly patient with chest pain, out of hospitalcardiacarrest and LBBB), and the Modified Sgarbossa Criteria confirms Occlusion MI in this case. But by this time the patient went into cardiogenicshock and passed away.
There was 100% proximal LAD occlusion with TIMI 0 flow, and cardiacarrest in the cath lab. The patient had a protracted hospitalization and did not survive. As often emphasized by Dr. Smith — sinus tachycardia is not a common finding with acute OMI unless something else is going on (ie, cardiogenicshock ).
An elderly man with sudden cardiogenicshock, diffuse ST depressions, and STE in aVR Literature 1. Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography. However, STE-aVR with multilead ST depression was associated with 31% in-hospital mortality compared with only 6.2%
Had such been the case, this patient would likely have been a prehospital cardiacarrest, or have been in profound cardiogenicshock at the time of ED arrival. The formal diagnosis codes were populated to the chart by the primary hospitalization teams. See Dr. Smith’s comments below.
The “weekend effect” is a well-documented phenomenon in hospital care, often linked to reduced staffing levels, leading to potential delays in diagnosis and intervention. Weekend procedures also face limited access to specialized cardiac teams, affecting timely decisions and making urgent procedures more difficult to schedule.
BACKGROUND:There are limited large-scale data on the outcomes of patients with cardiogenicshock (CS) transferred to hub centers. Overlap propensity score weighting was performed to assess the association between transfer status and in-hospital mortality. In-hospital mortality was lower in transferred patients39.1%
Figure B At this point, with the ECG changing from diffuse ST depression to widespread ST elevation and the patient presenting in cardiogenicshock, left main coronary artery (LMCA) occlusion is the likely diagnosis. This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent!
Predictors of weaning failure from veno-arterial extracorporeal membrane oxygenation (VA-ECMO) in patients with cardiogenicshock. The cause of CS was acute myocardial infarction in 438 (63.9%) patients, and 431 (62.9%) patients presented with cardiacarrest. RRT, renal replacement therapy. interquartile range 4.112.7]
BACKGROUND:In patients with ST-segment–elevation myocardial infarction complicated by cardiogenicshock, primary percutaneous coronary intervention (pPCI) is the preferred revascularization option. pharmacoinvasive and 46.2% pharmacoinvasive and 46.2% The incidence of the primary safety outcome was 10.1% 1.09];P=0.08).CONCLUSIONS:In
Lactate was 20, POC Cardiac US showed EF estimated at 30%, and formal echo showed EF of only 15%, and a normal RV. Assessment was severe sudden cardiogenicshock. 3 studied 416 patients hospitalized with COVID in China, of whom 82 had an initial cTn(I) above the upper reference limit. What is it? There is STE in V2-V6.
Aims Among patients with cardiogenicshock, immediate initiation of extracorporeal membrane oxygenation (ECMO) did not demonstrate any benefit at 30days. The present study evaluated 1-year clinical outcomes of the Extracorporeal Membrane Oxygenation in the therapy of CardiogenicShock (ECMO-CS) trial.
In fact, most do not make it to the hospital alive, which explains why only a tiny percent of OMI are due to full LM occlusion. Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiacarrest, cardiogenicshock or impending shock.
BackgroundVenoarterial extracorporeal membrane oxygenation (ECMO) provides full hemodynamic support for patients with cardiogenicshock, but optimal timing of ECMO initiation remains uncertain. Multivariable logistic regression evaluated the association between time from admission to ECMO initiation and in‐hospital death.
BackgroundPatients hospitalized with COVID19 from socioeconomically vulnerable communities are at risk for inhospital cardiovascular events. ConclusionsAmong survivors of COVID19 hospitalization, patientlevel social vulnerability was associated with cardiovascular events, explained by increased comorbidities.
There is limited understanding of race differences in the management and outcomes of CS.Methods:We queried the US National Inpatient Sample database (years 2016-2021) for CS hospitalizations in adults and categorized them by presence of acute myocardial infarction (AMI) on admission. 0.93), pLVAD (aOR: 0.79, 95%CI: 0.72-0.86),
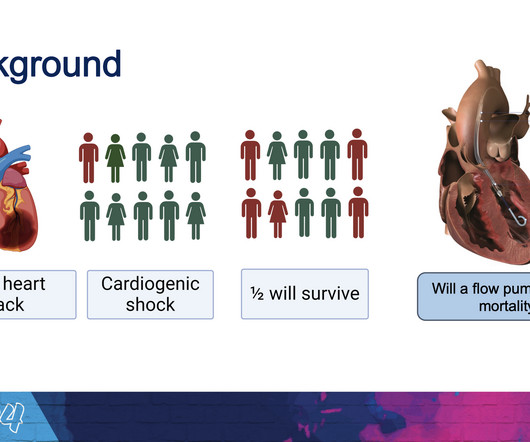
milla1cf Mon, 04/08/2024 - 18:07 April 8, 2024 — Implantation of the Impella CP micro-axial flow pump in the hours after a heart attack significantly increased the rate of survival at six months among people suffering cardiogenicshock, according to a study presented at the American College of Cardiology ’s Annual Scientific Session.
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. The patient was extubated on Day-3 of the hospital stay. The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker.
Discharging patients with NH-IMRangio<40 units at 48 hours after admission would reduce the total in-hospital stay by 943 days (median 2 [1–4] days per patient).CONCLUSIONS:NH-IMRangiois NH-IMRangioguided strategies to early discharge may contribute to safely shorten hospital stay, optimizing resources utilization.
This pattern is essentially always accompanied by cardiogenicshock and high rates of VT/VF arrest, etc. The patient arrived to the ED in cardiogenicshock but awake. Plus recommendations from a 5-member panel on cardiacarrest. in-hospital mortality was 18.8% Code STEMI was activated.
Risk prediction for cardiogenicshock patients with Impella. Abstract Aims Impella has become a new option for mechanical circulatory support in patients with cardiogenicshock (CS); however, prognostic models for patients after Impella are lacking.
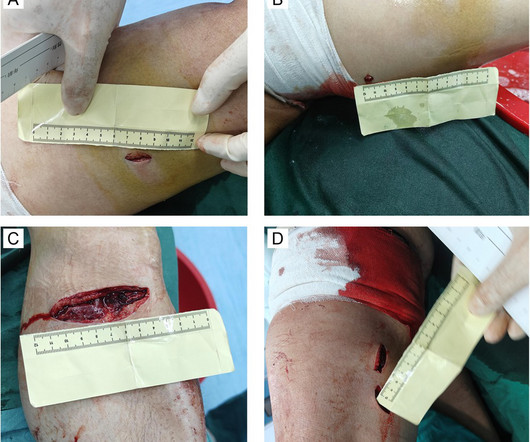
BackgroundTraumatic cardiacarrest (TCA) poses significant challenges in resuscitation, with extremely high mortality rates, making it a critical issue in emergency and critical care medicine. The patient experienced cardiacarrest upon admission to a local hospital.
1) as far as I can tell, there is very little data on amiodarone for this indication 2) amiodarone has beta blockade effects which could be deleterious in a patient with large anterior MI with pulmonary edema and at risk for cardiogenicshock (and she did go into shock. DOI: 10.1016/j.resuscitation.2025.110515
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content