This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A recent major review of data published by The Lancet and led by Emory sports cardiologist Jonathan Kim, MD, shows that Black athletes are approximately five times more likely to experience sudden cardiacarrest (SCA) and sudden cardiac death (SCD) compared to white athletes, despite some evidence of a decline in rates of SCD overall.
Curtain etal1 performed an analysis of the VALIANT (Valsartan in Acute Myocardial Infarction) and PARADISE-MI (Prospective ARNi vs ACE Inhibitor Trial to Determine Superiority in Reducing Heart Failure Events After MI) trials to evaluate whether risk of sudden cardiacarrest (SCA) following acute myocardial infarction (MI) has changed over time.
(MedPage Today) -- Despite concerns, there was no significant increase in sudden cardiacarrest (SCA) among young athletes during the COVID-19 pandemic, according to national surveillance data. Comparing prepandemic and pandemic periods, the numbers.
Designed to identify cardiacarrest events, the system can automatically place an emergency call when it senses an event has occurred, even if the user is unresponsive.
Sudden cardiacarrest may occur in various conditions when someone, while active (playing basketball or walking with friends), collapses and passes out. Their blood pressure drops, and often their heart stops. This may be caused by a lethal arrhythmia, which is when the heart beats abnormally and does not efficiently pump anymore.
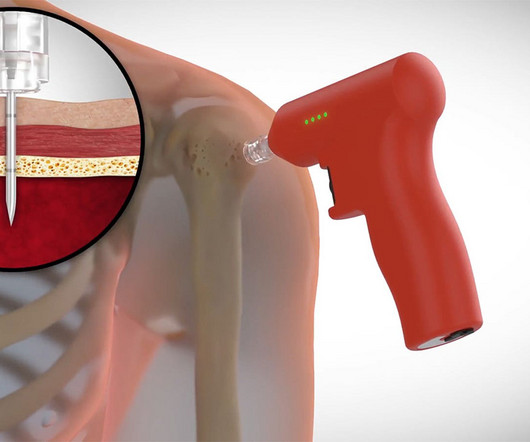
(MedPage Today) -- Intraosseous vascular access for the administration of epinephrine during out-of-hospital cardiacarrest wasn't better than going for the veins first, two separate randomized trials showed. In the PARAMEDIC-3 trial conducted.
In this report, we follow up on the resulting public interest on sudden cardiacarrest that made Hamlin the most searched person of 2023. (MedPage Today) -- In January, we reported on Damar Hamlin's collapse during a televised football game.
(MedPage Today) -- Therapeutic hypothermia did not improve survival or functional outcomes in unconscious patients after out-of-hospital cardiacarrest with initial nonshockable rhythm, a meta-analysis of patient-level data found. The primary.
The sooner a lay rescuer (bystander) starts cardiopulmonary resuscitation (CPR) on a person having a cardiacarrest at home or in public, up to 10 minutes after the arrest, the better the chances of survival and brain protection, according to an analysis of nearly 200,000 out-of-hospital cardiacarrest cases in the U.S.
Out-of-hospital cardiacarrest (OHCA) in people experiencing a heart attack is a time-dependent medical emergency requiring immediate cardiopulmonary resuscitation (CPR).
Research Highlights: The sooner a lay rescuer (bystander) starts cardiopulmonary resuscitation (CPR) on a person having a cardiacarrest at home or in public, up to. This news release contains updated information and data not included in the abstract.
Image courtesy of Takenobu Shimada, Osaka Metropolitan University (CC BY 4.0, [link] mtaschetta-millane Mon, 07/29/2024 - 09:09 July 29, 2024 — When it comes to treating cardiacarrest, acting quickly can mean the difference between life and death. Cardiacarrest can lead to death within minutes.
Moderate to severe anemia was linked to an increase in cardiacarrest or stroke compared with normal hemoglobin levels in critically ill COVID-19 patients.
Cardiacarrest is when the heart stops abruptly with little or no warning. According to American Heart Association data, 9 out of every 10 people who experience cardiacarrest outside of a hospital die. It is often fatal.
Research Highlights: An analysis of cardiacarrest records in a U.S. registry revealed that people with drug overdose cardiacarrests were more likely to be younger, have fewer health conditions and have higher survival rates with better neurologic.
Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. The morning before the cardiacarrest potassium was 4,3.mmol, After about 90 seconds of chest compressions she awoke.
Photo by Cedars-Sinai milla1cf Fri, 03/01/2024 - 08:25 March 1, 2024 — Two new studies by Cedars-Sinai investigators support using artificial intelligence (AI) to predict sudden cardiacarrest-a health emergency that in 90% of cases leads to death within minutes.
survival rates from out-of-hospital cardiacarrests fell significantly at the beginning of the COVID-19 pandemic in 2020 and only slightly. This news release contains updated information and data not included in the abstract. Research Highlights: U.S.
has no memory of his own cardiacarrest in 2016. He only knows that first responders resuscitated his heart with a shock from a defibrillator, ultimately leading to his complete recovery and putting him among fewer than one in 10 people nationwide who survive cardiacarrest outside of a hospital. Joshua Lupton, M.D.,
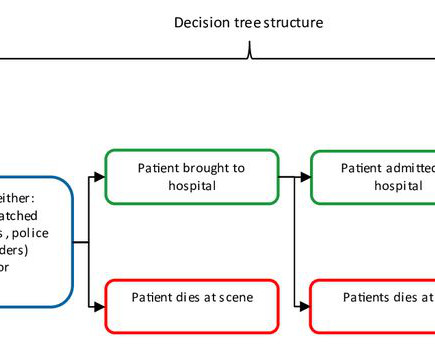
Objective Out-of-hospital cardiacarrest (OHCA) is a major public health challenge across Europe, with a survival rate of only 8.5% to hospital discharge. Implementing a community first responder (CFR) system, including earlier Basic Life Support and defibrillation, can enhance survival rates and neurological outcomes.
According to the American Heart Association, the world's leading nonprofit organization focused on heart and brain health for all, research shows that the exertion of shoveling snow may lead to an increased risk of a heart attack or sudden cardiacarrest.
Particularly, his contributions to the sudden cardiacarrest medical knowledge base have changed the way we think about this deadly condition that we might be able to prevent on a larger scale.” Although “sudden cardiacarrest” and “heart attack” are often mistaken to be the same, the conditions are quite different.
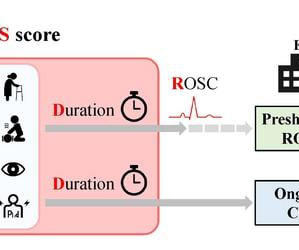
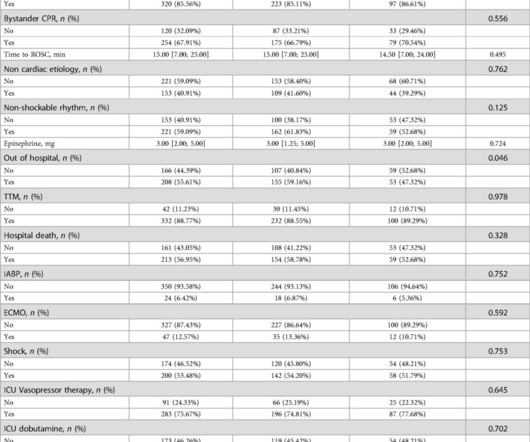
We identified variables linked to hospital mortality in the training set using Least Absolute Shrinkage and Selection Operator (LASSO) regression, as well as univariate and multivariate logistic analyses.
Despite improvements in CPR and rates of getting patients to the hospital, only about 10% of people ultimately survive after out-of-hospital cardiacarrest (OHCA), translating to about 300,000 deaths per year in the United States.
It is well known that acting quickly in the event of a cardiacarrest is important, but what does a quick initial shock with a defibrillator mean exactly for patients' chances of survival?
An analysis of data for more than 500,000 out-of-hospital cardiacarrests in the U.S. found key differences in outcomes between cardiacarrests caused by drug overdoses and cardiacarrests due to other causes, according to new research published today in the Journal of the American Heart Association.
Task forces comprising international experts in sports cardiology and the respective topics covered were assigned to each section and prepared specific clinical considerations tables for practitioners to reference.
Most cases of cardiacarrest during sport are likely to be preventable. In addition, the emergency response with cardiopulmonary resuscitation (CPR) and defibrillators within the sports context can be improved. This has been shown in a thesis from the University of Gothenburg.
People who experience out-of-hospital cardiacarrest often require care at a regional center for continued treatment after resuscitation, but many do not initially present to the hospital where they will be admitted. Circulation, Ahead of Print.
BackgroundGiven increases in drug overdose‐associated mortality, there is interest in better understanding of drug overdose out‐of‐hospital cardiacarrest (OHCA). Adjusted results showed comparable survival with Cerebral Performance Category score =1 or 2 when the first monitored arrest rhythm was shockable (OD: 28.9%
Researchers at Oregon Health & Science University have found that quality of care for pediatric patients who experience cardiacarrest outside of the hospital is lower compared with adults, prompting an urgent call to action to improve care delivery for the potentially deadly event.
This randomized trial showed no significant difference in return of spontaneous circulation between initial intraosseous and intravenous vascular access in adults with out-of-hospital cardiacarrest.
Sudden cardiacarrest (SCA) risk stratification in patients with mitral valve prolapse (MVP) may be complicated by other potential causes of arrhythmia.
In a trial involving adults with out-of-hospital cardiacarrest, an intraosseous-first strategy for vascular access did not result in a higher incidence of 30-day survival than an intravenous-first strategy.
A new observational study suggests the position in which responders initially place the two defibrillator pads on the body may make a significant difference in returning spontaneous blood circulation after shock from a defibrillator.
(MedPage Today) -- A familiar biomarker emerged as a potential predictor of sudden cardiacarrest (SCA) in young people, which remained hard to explain even with genetic testing. Although SCA was rare in a Korean population-based study -- occurring.
Out-of-hospital cardiacarrest survival rates dropped significantly at the onset of the COVID-19 pandemic in 2020 and have continued to remain lower than in the pre-pandemic years of 2015–2019, according to a preliminary study to be presented at the American Heart Association's Scientific Sessions 2024., 16–18, 2024, in Chicago.
Out-of-hospital cardiacarrest is a leading cause of death, accounting for ≈50% of all cardiovascular deaths. The cardiac catheterization laboratory plays an important role in the coordinated Chain of Survival for patients with out-of-hospital cardiacarrest. Circulation, Ahead of Print.
Updated Guideline Highlights: The American Heart Association and the American Academy of Pediatrics update recommendations for untrained lay rescuers and trained rescuers resuscitating adults and children who have drowned. One important update is the.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content