This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Traditional transvenous pacemakers consist of a pacemaker generator usually positioned surgically in the upper left chest on the pectoral muscle fascia and one or more leads positioned through the veins to the right atrium and across the tricuspid valve to the right ventricular apex.
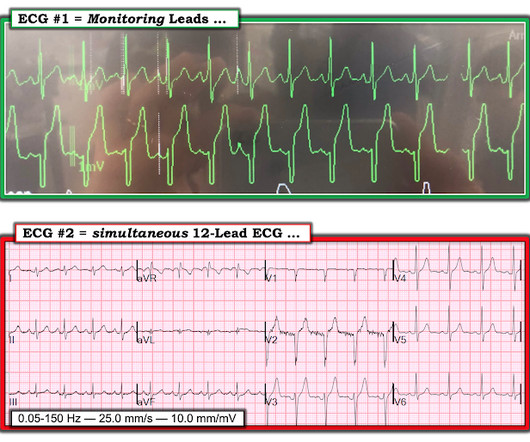
Physiologically — the most commonly observed pattern of AFlutter, known as " Typical " AFlutter — produces 2:1 negative deflections seen in the inferior leads ( as seen in Figure-3 ) — as a result of CCW ( C ounter C lock W ise ) rotation of a fixed reentrant circuit around the tricuspid valve annulus and through the cavo-tricuspid isthmus.
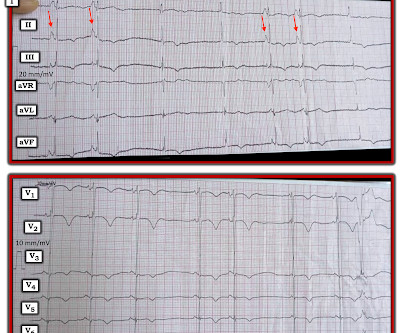
Perhaps the patient has pulmonary hypertension and/or tricuspid regurgitation? There definitel are periods of bradycardia (so pacing may be needed for that). Hope this helps — :) ECG-3 — I see sinus bradycardia and arrhythmia. RED arrows show what looks to be sinus P waves that are HUGE !!!!
In the new image on the right, it no longer turns upward within the atrium, but continues distally into the tricuspid valve or ventricle. This is supported by the PT note which described a palpably irregular pulse with pauses and marked bradycardia. In the old x-ray on the left, the lead appears to terminate within the atrium.
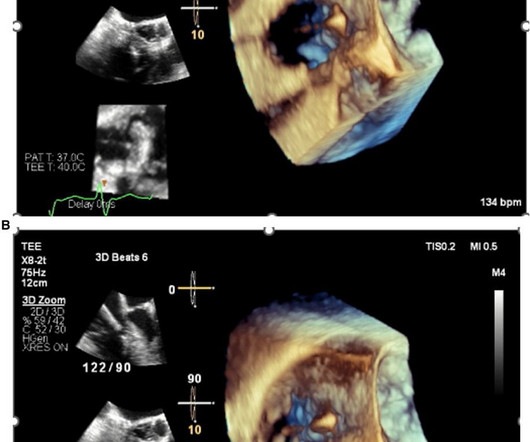
Tricuspid regurgitation jet velocity and pulmonary regurgitation end diastolic velocity indicating pulmonary hypertension are also taken as surrogates of left atrial pressure in the absence of pulmonary disease. Use of drugs producing bradycardia like beta blockers in stages III and IV may precipitate low output state.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









Let's personalize your content