This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There was concern that the rhythm might represent ventricular tachycardia, so lidocaine was given and one attempt at cardioversion was performed. See our other countless hyperkalemia cases below: General hyperkalemia cases: A 50s year old man with lightheadedness and bradycardia Patient with Dyspnea. A Very Wide Complex Tachycardia.
(MedPage Today) -- BOSTON -- A leadless pacemaker reliably communicated with a subcutaneous implantable cardioverter-defibrillator (S-ICD) to deliver anti-tachycardia (ATP) and bradycardia pacing, the MODULAR ATP study showed. In terms of safety.
Wireless implantable cardioverter-defibrillators (ICDs) eliminate the lead-related complications that come with a wired ICD, but they are unsuitable for patients with ventricular tachycardia, when the heart beats too quickly, or bradycardia, when the resting heart rate is seen as low.
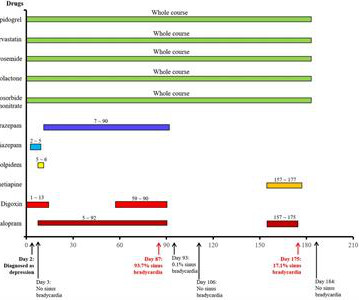
Here, a rare repeated sinus bradycardia event due to escitalopram is first reported. In an 82-year-old female patient with cardiac dysfunction using digoxin, tachycardia (average heart rate of 93 beats/min) was demonstrated by electrocardiogram (ECG). No other drug changes were made during these periods.
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. As described above by Dr. Smith Pacing in today's case is an effective intervention as doing so prevents the bradycardia and pauses that are likely to precipitate additional episodes of Torsades de Pointes. (
Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct. Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias.
The ECG shows an example of a patient with bradycardia/tachycardia syndrome. After a further pause of just under 2000 ms, 2 sinus node beats follow, which merge into a sinus tachycardia or atrial tachycardia (heart rate approx. Initially, a sinus rhythm with a heart rate of approx. 70 bpm is seen. 120 bpm here).
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
Typically, patients with HCM experience sinus tachycardia and sinus arrest relatively infrequently. To manage the complex comorbidities, we opted for dual-chamber pacemaker implantation.
Electrocardiogram (ECG) and telemetry revealed junctional bradycardia with heart rate in 30s and sinus pauses (5-7 seconds). He was admitted for further workup of bradycardia. His home medications included metoprolol succinate 25mg daily which was held given bradycardia. Initial laboratory analysis was unremarkable.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. For example — bradycardia and AV conduction disturbances are not uncommon with Hyperkalemia , with these conduction disturbances most often resolving once serum K+ is corrected. She was started on isoprenalin (isoproterenol).
During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia.
The ECG shows an example of a patient with bradycardia/tachycardia syndrome (also called sick sinus syndrome). After a further pause of just under 2000 ms, 2 sinus node beats follow, which merge into a sinus tachycardia or atrial tachycardia (heart rate approx. Initially, a sinus rhythm with a heart rate of approx.
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia. Ventricular tachycardia – more than 7 consecutive complexes originating from ventricles at a rate of > 100 bpm. Usually does not exceed 160 bpm.
Wide-complex tachycardia: VT or aberrant, or "other?" A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Sinus tachycardia with aberrancy was unlikely as the rate was consistently 150 bpm, without spontaneous variation. second ), in which the tachycardia is sustained.
Initially, there is an accelerated atrial rhythm/atrial tachycardia. Pre-automatic pause is a pause after a tachycardia and before an automatic rhythm, like sinus rhythm or, in this case, junctional escape rhythm. This EKG shows the classic features of sick sinus syndrome. Paper speed is 12.5
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ).
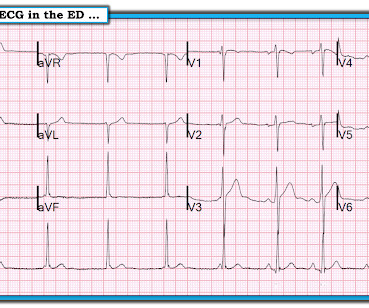
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. It is hard to make out P waves but you can see them best in V2, and notches in the T waves in other leads - this is a sinus tachycardia with a very long PR interval indicating first degree block.
RBBB is no longer seen after conversion to sinus rhythm — which supports our suspicion that the intermittent RBBB conduction seen every-other-beat during the tachycardia ( in Figure-1 ) was rate-related. Note that QRS morphology after conversion to sinus rhythm is very similar to QRS morphology of odd-numbered beats during the tachycardia.
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
Sometimes, head up tilt test, also known in short as HUTT, is also done for the evaluation of postural orthostatic tachycardia syndrome, POTS, a condition in which there is tachycardia on standing up, without a fall in blood pressure. Second is cardioinhibitory response, in which there is bradycardia, but no hypotension.
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). He required multiple defibrillations within a period of a few hours.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical. Early Detection of Issues Wearable devices provide real-time alerts about irregularities in heart function.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
This is often secondary to sinus tachycardia, sinus bradycardia and sinus arrhythmia, or isolated premature atrial or ventricular arrhythmias (VAs). To be aware of important medication contraindications during pregnancy and lactation, as they pertain to arrhythmia management and anticoagulation. 2–4.
during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Thus, there is sinus bradycardia and arrhythmia sinus pauses ( which may be longlasting, ultimately leading to sinus arrest ) and SA nodal block. The indication for pacemaker placement with SSS is symptomatic bradycardia.
Descriptive analysis of the ECG in today's case reveals a regular, narrow tachycardia at ~130/minute , without clear sign of sinus P waves. But the rate is ~130/minute — which is a bit fast for sinus tachycardia. So IF this is sinus tachycardia with a sinoventricular rhythm — then we have to explain WHY the rate is this fast.
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management Cardiac Arrest. Is it STEMI?
Abstract Introduction Severe transitory episodes of bradycardia with subsequent syncope in children are common, and generally portend a benign prognosis. with one documented SP after termination of atrial tachycardia at the 3-month follow-up. The median longest pause was 8.9 s s (range 3.9–16.8) s (range 0.8–2.2)
We have borderline sinus bradycardia with 1 ° AVB and occasional PACs. If this was a tachycardia at a rate of 150, it might appear to be a narrow complex tachycardia, when in fact, it would be a wide complex tachycardia! ECG diagnosis: Borderline sinus bradycardia, 1st degree AVB, RBBB, and occasional PACs.
There is a regular, wide complex, (mostly) monomorphic tachycardia. The differential of wide, regular, monomorphic tachycardia is: VT or SVT with aberrancy, all +/- hyperkalemia (see diagrams below). Really wide tachycardia = VT or SVT with conduction abnormality + hyperkalemia, until proven otherwise.
After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. ST elevation in aVL with reciprocal ST depression in the inferior leads Shock, bradycardia, ST Elevation in V1 and V2. He also received insulin with D50, sodium bicarbonate, and kayexalate for hyperkalemia.
A rapid heartbeat (tachycardia) can increase the workload on your heart, while a slow heartbeat (bradycardia) can cause fatigue and dizziness. It’s crucial to monitor your blood pressure regularly and report any significant changes to your healthcare provider so they can adjust the dosage of the medication accordingly.
This phenomenon is best known as, A V D issociation b y D efault ie, default of the sinus pacemaker due to marked sinus bradycardia, which transiently allows the AV nodal escape pacemaker to take over. Instead, as we state above the rhythm is sinus bradycardia with marked sinus arrhythmia. Close follow-up is essential.
As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ). There is marked, diffuse ST segment depression in ECG #1.
I completely agree with Dr. Nossen that in this patient with new CP and sinus tachycardia with LAHB — that the T waves in each of the inferior leads are hyperacute ( ie, clearly disproportionately "bulky" given size of the QRS in these leads ). — and which other patient(s) need to be seen as soon as possible to figure out what is going on?
As a result, rather than atrial tachycardia — I suspect we are seeing a slightly increased sinus rate with the above described 2nd-degree dual-level AV block. As a result, if significant bradycardia persists ( especially if accompanied by symptoms ) — then pacing may be needed.
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. The novel technology system present in 12L ECG helps us analyze unrecognizable ECG patterns that are hard to detect by human eyes.
Other than tachycardia, Other than slight tachycardia, vitals were within normal limits (including oxygen saturation). The rhythm in ECG #1 is sinus tachycardia at 115-120/minute. There is still sinus tachycardia in ECG #2 — although the heart rate has now slowed to ~100/minute. Apparently he denied chest pain.
Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. The most common triggered arrhythmia is Torsades de Pointes. But the sinus node works on automatic activity, as do all escape rhythms. Do not treat AIVR. In fact, use of antidyrhythimcs (e.g.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content