This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
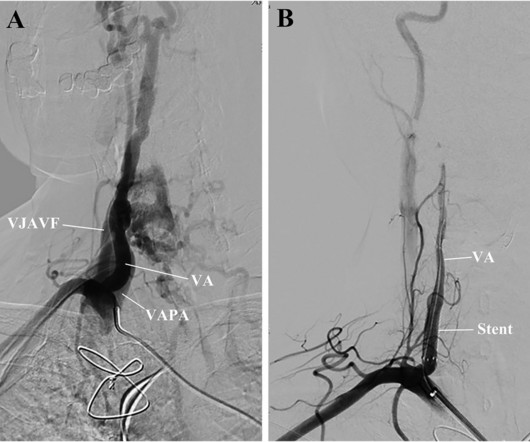
The patient, who complained of dizziness, was initially diagnosed with bradycardia and aortic paravalvular leak. Using the endovascular technique, a 4mm stent graft was deployed in a 3.6mm VA to cover both the VJAVF and the VAPA ostia. A VAPA originated from another ostium of the right VA without a drainage vessel.
OBJECTIVECarotid artery stenting for heavily calcified lesions is challenging for interventionists. Sufficient dilatation was achieved, followed by carotid stent deployment (Precise Pro RX; Cordis, Miami Lakes, FL, USA). Stroke: Vascular and Interventional Neurology, Ahead of Print.
There’s competing sinus bradycardia and junctional rhythm, with otherwise normal conduction, borderline right axis, normal R wave progression and voltages. Cath lab was activated, and found a 95% proximal LAD occlusion which was stented. Significant bradycardia ( rate in the 40s/minute ) — is present throughout.
Former resident: "Just saw cath report, LAD stent was 100% acutely occluded." They of course opened and stented it. They said it looked similar to his old one (in my opinion, similar, but not similar enough to be able to say no OMI)." Smith : "What was the outcome?" You taught us well!"
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. preceding each of the fascicular beats — indicating a faster rate for the escape rhythm compared to the sinus bradycardia ).
Case continued Another ECG was recorded 3 hours later, still 1/10 pain: There is sinus bradycardia with RBBB. The culprit was opened and stented. They only mask the underlying pathology. Aspirin and heparin were given, but no NTG. There is minimal STE in I and aVL, but this can be quite normal in RBBB.
The ECG shows sinus bradycardia but is otherwise normal. On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions. OM before and after, arrow indicating stented region. The following ECG was obtained.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. It was stented. He wrote most of it and I (Smith) edited.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chest pain. The computer called "Sinus Bradycardia" only (implying that everything else is normal. The overreading Cardiologist called it only "Sinus Bradycardia" with no other findings. The rhythm in Figure-1 is sinus bradycardia and arrhythmia.
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. C ASE C onclusion : Timely cardiac cath was performed on today's patient — with successful reperfusion and stenting of his proximal LAD occlusion. = The PR and QRS intervals are both normal.
Here is his ED ECG: There is bradycardia with a junctional escape. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. He appeared gray in color, with cool skin. What is the atrial activity?
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. No appreciable skin pallor. He reported to be a social drinker, but used tobacco products daily. Here is the time-zero 12 Lead ECG.
Here are inferior leads, and aVL, magnified: A closer inspection of the inferior leads and aVL Sinus bradycardia. The patient was then taken to the cath lab an found to have a proximal RCA 100% thrombotic occlusion which was successfully stented. I had no history on the case and no prior ECG for comparison. What do you think?
60-something with h/o MI and stents presented with chest pain radiating to the back and nausea/vomiting. It was stented. The patient had a p rior h istory of MI + stents. This is sinus bradycardia. Time zero What do you think? There is inferior ST elevation. Is it normal variant? Is it ischemic (OMI)? Pericarditis?
After many hours, the decided that it was appropriate to do an angiogram and they found a distal LAD occlusion which was opened and stented. Patient presentation is important This was a 60-something with acute chest pain: There is sinus bradycardia at a rate of 44. Why bradycardia? It was stented. STE60V3 = 2.5
Here is his previous ECG: This was my interpretation of the first ECG: Sinus bradycardia with less than 1mm ST elevation in V4-V6, elevated compared to the previous ECG, suggestive of lateral MI. Both were stented. This is his first ECG in the department, which I saw as it was being printed: What do you think?
They had a history of non-ischemic cardiomyopathy (EF 30%), as well as PCI with one stent. These include not only induction of significant bradycardia ( albeit usually short-lived ) — but also both ventricular and supraventricular tachyarrhythmias. Home medications included metoprolol, but no calcium- or sodium-channel blocking agents.
Stent placed. The rhythm in ECG #1 is sinus bradycardia and arrhythmia. : Now it is not subtle: there is clear, obvious inferior posterior OMI. At this point, the cath lab was activated. Angiography showed: 100% Distal RCA occlusion. Pre- procedure TIMI 0 flow was noted. Post Procedure TIMI III flow was present.
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. What do you think?
She was taken to cath and found to have total mid RCA occlusion, TIMI 0 flow, stented with excellent result. Obvious STEMI(+) OMI of inferior, posterior, and lateral walls, now with likely 2nd degree heart block type 1 (Wenckebach). Finally the OMI was realized. Her heart block resolved quickly. Echo showed matching wall motion abnormalities.
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
The role of intracranial stenting in ICAS remains uncertain. In the SAMMPRIS trial, patients who had experienced recent TIA/CVA secondary to 70‐99% ICAS demonstrated an increased risk of recurrent stroke when treated with angioplasty and stenting compared to medical therapy alone [1].
He has a h/o of 3 vessel disease and stents and his pain has been on and off for days. MY Thoughts on the ECG in Figure-1: The rhythm in ECG #1 is sinus bradycardia at ~50-55/minute. Even if the Queen says Not OMI with High Confidence, you should get serial ECGs in a patient who has a high pretest probability. No chamber enlargement.
The patient was referred immediately for cath which revealed RCA occlusion that was stented. There is some down sloping ST-segment and T wave inversion in lead aVL. The findings are diagnostic of inferior and posterior wall OMI. How did the Queen of Heart AI model perform? True Positive ECG#2 : Also sinus rhythm.
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. This was stented. The corrected QT interval is extremely long, about 500 ms.
Soon afterward, the patient’s symptoms return along with lightheadedness, bradycardia, and hypotension. The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. Two stents were placed with resultant TIMI 3 flow.
His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. The lesion was successfully stented. Blood pressure: 130/80 mmHg, heart rate: 45/min, respiratory rate: 18/min, SaO2: %98, body temperature: normal. As he seemed very agitated, fentanyl and diazepam were given. No reciprocal ST-segment depression (STD). --QT
Patient 2 : 55 year old with 5 hours of chest pain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Smith : The fact that the ECG did not evolve is further proof that this was the baseline ECG. nearly identical to the first case).
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. He had a 100% RCA occlusion which was stented.
Here is the cath report (TIMI-2 flow in the circumflex -- stented): Learning Point: Just because the cardiologist says it is "not a STEMI" and "wants to teach you about the ECG", it does not mean you should back down. The rhythm is sinus bradycardia at ~55-60/minute. They do not recognize these patterns. What are the ECG Findings?
His rhythm on telemetry seemed to be sinus bradycardia vs junctional rhythm. Telemetry initially was interpreted as showing sinus bradycardia vs a junctional rhythm. A quick POCUS which showed significantly reduced ejection fraction and trace B lines. What do you think? The estimated left ventricular ejection fraction is 40-45%.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. After stent placement: The vessel is now open with TIMI 3 flow, although it is diffusely diseased and the middle segment is ectatic. The troponin peaked at 0.4
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content