This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Methods Consecutive patients with bradycardia indicated for pacing from 2016 to 2022 were prospectively followed for the clinical endpoints of heart failure (HF)-hospitalizations and all-cause mortality at 2 years. CSP should be preferred over VSP or RVP during pacing for bradycardia.
While weight loss following bariatric surgery often yields resolution of comorbidities related to obesity, it also presents unanticipated changes in underlying physiology. We present a case series of two young patients with obesity-related comorbidities necessitating sleeve gastrectomy which provoked symptomatic sinus bradycardia.
Welcome to the Physiology Friday newsletter. Physiologically Speaking is a reader-supported publication. This irregular sleep pattern misaligns circadian rhythms and disrupts physiology. ICYMI: On Wednesday, I published my video interview with Dr. Andrew Koutnik. “The shorter your sleep, the shorter your life.”
Conduction system pacing (CSP), including both left bundle branch area pacing (LBBAP) and His-bundle pacing (HBP) has been proposed as an alternative therapy option for patients with indication for cardiac pacing to treat bradycardia or heart failure.
Then, the current flows to an area known as the bundle of His, which divides into two branches (LBB and RBB) and is the only physiological pathway connecting the atria with the ventricles. Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia. Usually does not exceed 160 bpm.
The Role of Wearable Technology in Heart Health Wearable tech is designed to monitor physiological data and provide actionable insights to users. Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical.
Abstract Introduction Left bundle branch pacing (LBBP) is a physiological pacing modality. However, the long procedure and fluoroscopy time of LBBP is still a problem. This study aims to compare the clinical outcomes between transthoracic echocardiography (TTE)- and X-ray-guided LBBP.
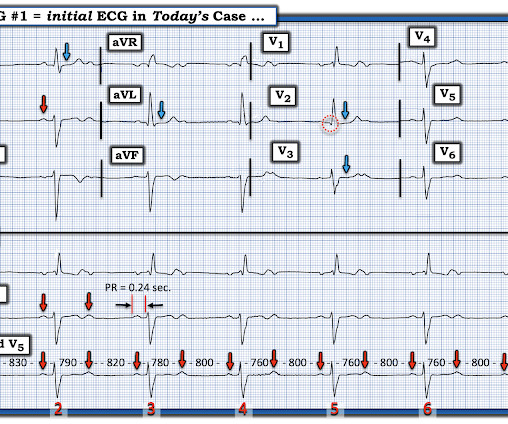
The rhythm is sinus bradycardia at a rate just over 50/minute. Figure-2: The repeat ECG in today's case — recorded as soon as the treating clinician recognized the lead misplacement. ( To improve visualization — I've digitized the original ECG using PMcardio ). All intervals ( PR,QRS,QTc ) are normal.
Physiologically — the most commonly observed pattern of AFlutter, known as " Typical " AFlutter — produces 2:1 negative deflections seen in the inferior leads ( as seen in Figure-3 ) — as a result of CCW ( C ounter C lock W ise ) rotation of a fixed reentrant circuit around the tricuspid valve annulus and through the cavo-tricuspid isthmus.
It is a physiological adaptation helping athletes perform physical tasks better than non-athletes. Athlete’s bradycardia due to increased parasympathetic tone and decreased sympathetic tone is a well-known observation. The upper limit of physiologic cardiac hypertrophy in highly trained elite athletes. References 1.Prior
The ECG shows sinus bradycardia but is otherwise normal. Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The documentation does not describe any additional details of the history. The following ECG was obtained. ECG 1 What do you think?
Another factor to be considered, according to Chou’s textbook, is that many patients have dual AVN physiology and conduction is preferential down the fast pathway. This was all very alarming because his baseline routine, otherwise, is unencumbered as he reports a usually high exertional tolerance.
In other cases, the bypass tracts conduct intermittently, depending upon other factors such as cardioactive medication use, physiological stressors with catecholamine release, the development of coronary ischemia, and normal aging.”[3] Delta waves are seen in 11/12 leads.
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. The QRS complex in ECG #1 is wide.
The rule of thumb is less accurate, and the risk is higher because a long QT in the presence of bradycardia ("pause dependent" Torsades) predisposes to Torsades. 6) Use a different rule of thumb for bradycardia : Manually approximate both the QT and the RR interval. 3) At heart rates below 60, far more caution is due. Malik et al.
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
If there is PR prolongation from one to the next, this supports Mobitz I physiology which rarely benefits from pacing. Conversely, if the PR interval is constant , this supports Mobitz II physiology, which is an indication for pacing. This pattern can be seen in both Mobitz I and Mobitz II physiology. History is often helpful.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. Clearly the physiologic chain reaction of autonomic dysfunction seen in todays case does not commonly lead to death of the person learning this news. I do not know the answer to this.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content