This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
To manage the complex comorbidities, we opted for dual-chamber pacemaker implantation. Meanwhile, a dual-chamber pacemaker can treat HCM by changing the sequence of myocardial contraction. Subsequent examinations and follow-up revealed that pacing significantly reduced LVOT obstruction and corrected heart rhythm.
BackgroundThere have been few instances of symptomatic bradycardia-arrhythmia in the context of area postrema syndrome (APS), and some of them have been implanted permanent pacemakers. Brady-arrhythmia was presented in all patients, and 9 patients were implanted temporary or permanent pacemakers.
Men who perform well in the cross-country ski race Vasaloppet are at increased risk of having abnormally low heart rates and pacemakers later in life. However, the researchers behind the study did not uncover any link to increased mortality, rather the opposite—the skiers lived longer than the general population.
milla1cf Thu, 06/20/2024 - 19:40 June 20, 2024 — A programing algorithm, being tested by HonorHealth Research Institute for those patients with new or recently installed pacemakers, is designed so the device not only provides a steady heartbeat, but also controls high blood pressure.
The BACKBEAT pivotal study will evaluate the efficacy and safety of atrioventricular interval modulation (“AVIM”) therapy (also known as BackBeat CNT), for the treatment of pacemaker-indicated patients with uncontrolled hypertension despite the use of antihypertensive medications. Orchestra BioMed and Medtronic, Inc. Kowal, M.D.,
Does prolonged, high-intensity endurance training increase the risk of bradycardia requiring pacemaker implantation and ultimately the long-term mortality risk?
This can include our hearts, which may develop conditions like bradycardia or a slow heart rate. What Is Bradycardia ? Are you wondering “ What is bradycardia ?” Bradycardia is a condition in which the heart’s rhythm is too slow. Medications – Certain medications can slow down the heart rate as a side effect.
What happens to PR Interval in sinus Bradycardia ? Depends on the cause of Sinus bradycardia Answer When cardiac cycle slows down, every interval must get prolonged. Normally PR doesn,t stretch that far in isolated benign sinus bradycardia. Sinus rate is determined by SA nodal, funny pacemaker current (if).The
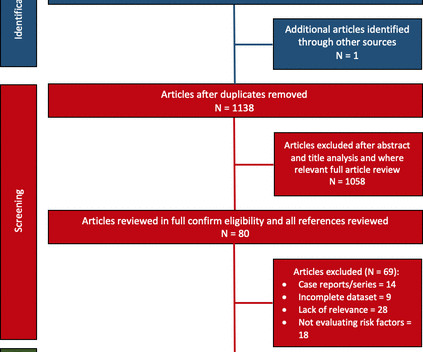
Objective We conducted a systematic review evaluating AF burden and bradycardia requiring permanent pacemaker (PPM) implantation and report any predictive risk factors identified. Study outcomes included AF or bradycardia requiring therapy. Databases included Embase, Medline, PubMed, Web of Science, CINAHL and Cochrane.
(MedPage Today) -- BOSTON -- A leadless pacemaker reliably communicated with a subcutaneous implantable cardioverter-defibrillator (S-ICD) to deliver anti-tachycardia (ATP) and bradycardia pacing, the MODULAR ATP study showed. In terms of safety.
Traditional transvenous pacemakers consist of a pacemaker generator usually positioned surgically in the upper left chest on the pectoral muscle fascia and one or more leads positioned through the veins to the right atrium and across the tricuspid valve to the right ventricular apex.
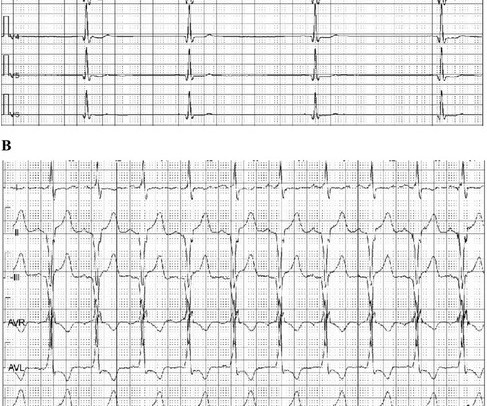
It comes from a pacemaker patient whose pacemaker was briefly switched to VVI at 30 bpm due to a stimulation threshold test. Let's analyze the ECG. The first 3 beats show a sinus rhythm with a frequency of approx. This is followed by a premature ventricular contraction (PVC).
Crew notifies the received ED of an incoming post-arrest patient and notes a sinus bradycardia on their monitor, as seen in Figure 2. Figure 2 : This rhythm shows a sinus bradycardia at a rate between 30 and 40bpm. The crew immediately initiated TCP at a rate of 70bpm and slowly increased the current, as shown in Figure 3.
I tell the residents: "The pacemaker is just common sense: if there is no beat, it provides one; if there is one, it keeps itself from pacing." This is similar to Ken Grauer's comment at the bottom: "What would I do if I were a pacemaker?" This made me realize that pacemaker function is not as well understood as I thought.
Methods Consecutive patients with bradycardia indicated for pacing from 2016 to 2022 were prospectively followed for the clinical endpoints of heart failure (HF)-hospitalizations and all-cause mortality at 2 years. CSP should be preferred over VSP or RVP during pacing for bradycardia.
Intravascular cardiac pacemakers are an established therapy for bradycardia. Recently, a new class of leadless pacemakers have mitigated some of the complications related to pacemaker leads.
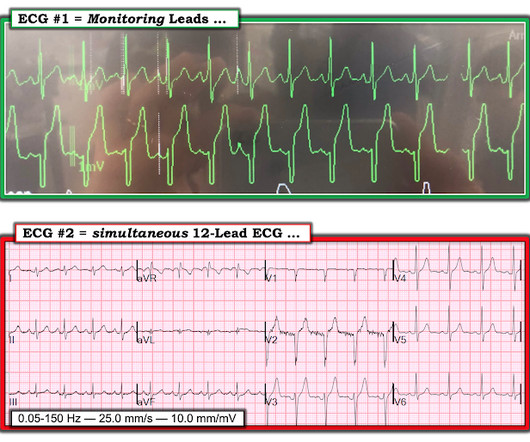
My thoughts were the following: ECGs #1 and #2 showed a completely unreliable sinus pacemaker, with presumed high-grade 2nd-degree AV block — and frequent resultant pauses of over 2 seconds ( that would have been even longer had it not been for intermittent relief from the atrial escape focus ). What Does this All Mean?
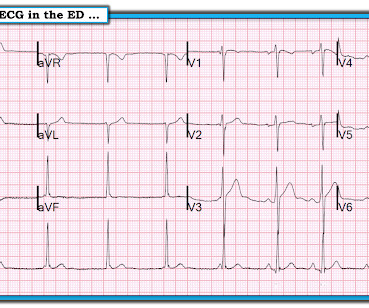
The ECG shows an example of a patient with bradycardia/tachycardia syndrome. Patients with bradycardia/tachycardia syndrome usually require a heart pacemaker to prevent the heart rate from becoming too slow. Initially, a sinus rhythm with a heart rate of approx. 70 bpm is seen. 120 bpm here). 120 bpm here).
The 2nd human genetically-modified cardiac xenotransplant occurred 9/20/23 at the University of Maryland with patient requiring placement of a permanent pacemaker on post-op day three for low cardiac output with relative bradycardia. After multi-disciplinary discussion the decision was made to proceed with an epicardial approach.
Written by Willy Frick A man in his 70s with a history of HFrEF and sick sinus syndrome s/p dual chamber pacemaker placement was admitted for overnight observation following outpatient placement of a mitral valve clip. This is unambiguous evidence of pacemaker malfunction. Imagine the pacemaker is set at a minimum rate of 60.
The implantation of leadless pacemakers has grown in recent years for the management of bradycardias. There are no randomized controlled trials to evaluate outcomes for single-chamber transvenous (TV), dual-chamber TV, and leadless pacemakers.
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Place temporary pacemaker 3. There is ventricular bigeminy with bizarre appearing wide T-waves See even more striking cases of this at the bottom of the post. The plan: 1.
Introduction: Leadless pacemakers (LP) are increasingly utilized in pts with bradycardia and may be associated with better outcomes compared to right ventricular pacing (RVP). Conduction system pacing (CSP) with HBP or LBBAP have been associated with reduction in death or heart failure hospitalization (HFH).
The following are key points to remember from a review article on cardiac implantable electronic devices (CIEDs), which include pacemakers for bradycardia, biventricular pacemakers for heart failure, and implantable cardioverter–defibrillators (ICDs) for the treatment of sudden cardiac death:
Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. She was intubated and a transvenous pacemaker was inserted with good capture. In addition to marked bradycardia — could there be high-grade AV block? Atropine produced no response. She received PR aspirin.
If the patient is showing signs of poor perfusion, we would stop here and prepare to increase the rate with a temporary pacemaker (transvenous or transcutaneous). There is no P wave in front of each QRS, so this is not sinus bradycardia. Why is the rate so slow?
Is a novel modular pacing–defibrillator system, consisting of a leadless pacemaker in wireless communication with a subcutaneous implantable cardioverter–defibrillator (ICD), able to effectively and safely provide antitachycardia and bradycardia pacing?
Left bundle branch block (LBBB) is a frequent complication of transcatheter aortic valve implantation (TAVI) and was shown to predict advanced atrio-ventricular block and pacemaker implantation (PI).1,2 1,2 Previous studies focused on persistent TAVI-induced LBBB. There are limited data on TAVI-related intermittent LBBB.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. They knew she would need a pacemaker unless some transient and reversible cause was discovered. Once this happens, of course, the patient will require temporary or permanent pacemaker as soon as possible.
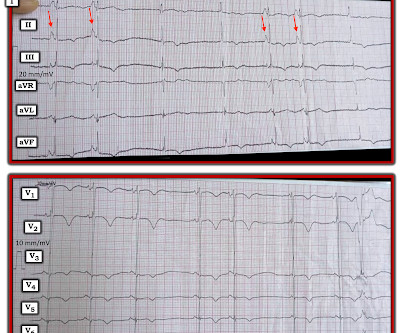
This is demonstrated ( Figure 5 ) by the gap in arrows at the bottom of the strip, signifying that the demand pacemaker has recognized an underlying rhythm (in this case, artifact from a moving ambulance). The artifact fools the pacemaker into thinking the rhythm is native.
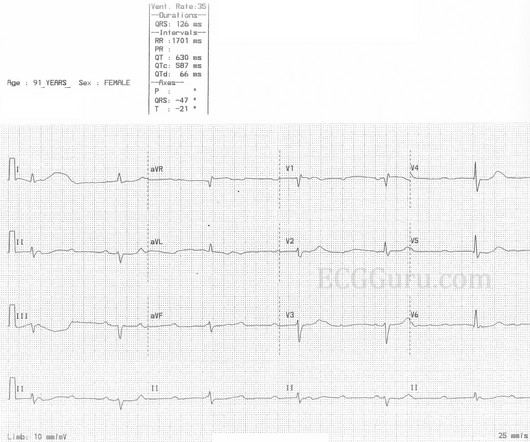
Is a pacemaker needed? Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
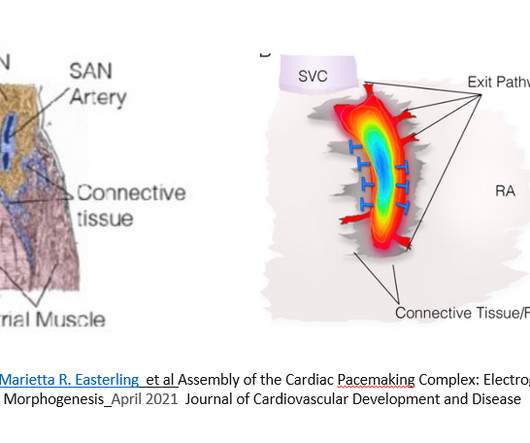
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia.
We admitted him for probable EP study and possible pacemaker. He underwent pacemaker placement and is doing fine. SSS is by far the most common reason for permanent pacemaker placement. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Learning Points: 1.
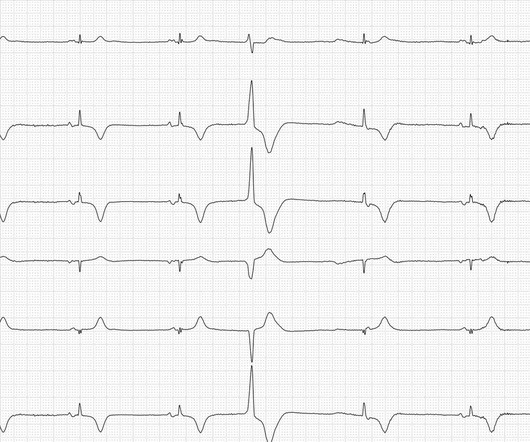
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. The patient may need a pacemaker. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. =
A newborn male was delivered via cesarean section at term due to acute fetal distress and fetal bradycardia, necessitating emergency pacemaker implantation. Physical examination revealed dysmorphic facial features and syndactyly in both upper and lower limbs.
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. preceding each of the fascicular beats — indicating a faster rate for the escape rhythm compared to the sinus bradycardia ).
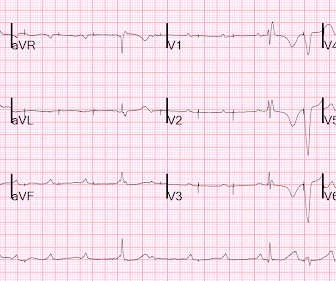
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study. be regular! —
There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
As a result of slowing of the sinus pacemaker the sinus rate occasionally drops below the intrinsic rate of the AV nodal escape pacemaker. Instead, as we state above the rhythm is sinus bradycardia with marked sinus arrhythmia. We emphasize the following KEY points: The rhythm in Figure-3 is not AV dissociation.
I’d guess the overall rhythm is sinus, perhaps with a wandering atrial pacemaker and very frequent ventricular ectopy with multiple couplets. In the meantime, a pacemaker may be needed. = There definitel are periods of bradycardia (so pacing may be needed for that).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content