This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
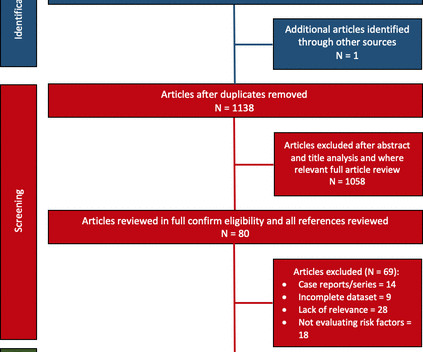
Objective We conducted a systematic review evaluating AF burden and bradycardia requiring permanent pacemaker (PPM) implantation and report any predictive risk factors identified. Study outcomes included AF or bradycardia requiring therapy. Databases included Embase, Medline, PubMed, Web of Science, CINAHL and Cochrane.
Abstract Introduction Clinical outcomes of long-term ventricular septal pacing (VSP) without His-Purkinje capture remain unknown. This study evaluated the differences in clinical outcomes between conduction system pacing (CSP), VSP, and right ventricular pacing (RVP).
The primary outcome was ventricular arrhythmias, the secondary outcomes were bradycardia and atrial fibrillation (AF).ResultsOur 0.66], but increased the risk of in-hospital bradycardia (OR 2.88, 95% CI 1.02–8.17) 8.17) compared with propofol.
Introduction: Leadless pacemakers (LP) are increasingly utilized in pts with bradycardia and may be associated with better outcomes compared to right ventricular pacing (RVP). The aim of the study is to assess the clinical outcomes in pts with LP compared to single chamber RVP and CSP.
This study aims to compare the clinical outcomes between transthoracic echocardiography (TTE)- and X-ray-guided LBBP. Abstract Introduction Left bundle branch pacing (LBBP) is a physiological pacing modality. However, the long procedure and fluoroscopy time of LBBP is still a problem.
This combination is often extremely effective for maintaining good longterm outcome ( Lanza and Shimokawa — Eur Cardiol 18: e38, 2023 ). In fact, the ECG was described as normal, and without serial ECGs or prior ECGs for comparison it could be. Initial high sensitivity troponin I returned at 6ng/L (normal 0.20
While these devices reduce symptoms and improve survival among patients with symptomatic bradycardia, they are associated with an increased risk of infection, venous occlusion, heart failure, and tricuspid valve regurgitation. A personalized approach to selecting the appropriate pacemaker for each patient is needed to optimize outcomes.
The implantation of leadless pacemakers has grown in recent years for the management of bradycardias. There are no randomized controlled trials to evaluate outcomes for single-chamber transvenous (TV), dual-chamber TV, and leadless pacemakers.
I did not think that the T-waves in V2 and V3 are hyperacute and I still do not--I disagree with Ken below--I think they are normal , especially in the context of bradycardia. Their apparently excessive length (QT interval) is due to bradycardia. They do not have much bulk. A corrected QT would be normal.
By understanding the nuances of abnormalities detected in Cardiomatics and interpreting detailed reports, healthcare professionals can intervene promptly to prevent adverse outcomes. Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia. In healthy individuals occurs during exercising or strong emotions.
This blog explores the ways wearable technology can help track heart health, the advantages it offers, and how it contributes to better outcomes for those requiring surgical intervention. Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical.
Syncope without prodrome is a significant risk factor for cardiac syncope and poor outcome. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Many patients have a T achy- B rady syndrome in which tachyarrhythmias ( most commonly rapid AFib ) alternate with periods of bradycardia.
The purpose of this case series is to provide an overview of the procedural and clinical outcomes of patients who underwent stenting for symptomatic ICAS.MethodsWe reviewed a database of all interventional procedures conducted at our institution to identify patients who underwent intracranial stenting from 2013 and 2022 for symptomatic ICAS.
Abstract Background Programed ventricular stimulation (PVS) is a risk stratification tool in patients at risk for adverse arrhythmia outcomes. years during which 14 patients (18%) experienced VA requiring treatment ( n = 14) or syncope due to bradycardia ( n = 2). Patients were followed for 1.6 ± 1.5 95% confidence interval: [1.2–27],
During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. This is what T-waves look like when there is a long QT." Below are two ECGs from the telemetry monitoring.
Conduction system pacing has gained popularity for bradycardia and cardiac resynchronization therapy indications. Left bundle branch area pacing (LBBAP) is a more straightforward technique with better long term outcomes compared to His bundle pacing.1
The patient was ultimately discharged with a poor neurologic outcome. Learning points: TCP is primarily recommended for bradycardia that does not respond to atropine, or other agents. The patient did have massive pulmonary emboli, but he also had profound intraventricular and subarachnoid hemorrhages.
Outcome and Analysis: ECG 1 is diagnostic of inferior and right ventricular MI. There is a junctional bradycardia. After midnight (now day 3), she complains of shoulder pain and dyspnea. Troponin was repeated and returned higher still. She was taken to the cath lab. What was the diagnosis?
Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury. Sinus Tachycardia ( common in any trauma patient. ).
Smith : "What was the outcome?" Former Resident: "They took him but they rolled their eyes at me (Smith editorial comment: how often have they rolled their eyes at YOU?). They said it looked similar to his old one (in my opinion, similar, but not similar enough to be able to say no OMI)." They of course opened and stented it.
Reflex syncope is defined as a transient loss of consciousness due to a neurally mediated reflex causing sudden-onset vasodilation and bradycardia, leading to a steep decrease in blood pressure and cerebral hypoperfusion. Thus, once the aetiology is established, further diagnostic tests are seldom performed.
A calcium burden is associated with suboptimal dilatation, periprocedural complications, high rates of restenosis, and poor outcomes. Although 1 patient experienced prolonged bradycardia and hypotension, they were well managed with anticholinergic and vasoconstrictive agents.
However, none of the formulas have proven to be definitively better than another and none are well correlated with outcomes or events! The rule of thumb is less accurate, and the risk is higher because a long QT in the presence of bradycardia ("pause dependent" Torsades) predisposes to Torsades. Measure it manually.
I sent it to 5 of my OMI friends without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: "reperfused inferior OMI". MY Thoughts on the ECG in Figure-1: The rhythm in ECG #1 is sinus bradycardia at ~50-55/minute. There is ischemic ST depression in V4-V6. No chamber enlargement.
ABSTRACT Introduction Leadless pacemakers (LPs) are a valuable treatment for bradycardia, with the Aveir offering advanced features, including a protective sleeve and active fixation.
A nightly sleep duration less than 6 hours per night appears to be especially detrimental, but some studies have even shown worse health outcomes for adults sleeping 7 hours or less compared to those sleeping the recommended 7–9 hours per night. The impact of optimizing circadian biology on health cannot be understated.
“Our collaboration with Orchestra BioMed will explore how cardiac pacing can go beyond management of bradycardia and conduction disease to treat hypertension as well,” said Robert C. Kowal, M.D., vice president and general manager of Cardiac Pacing Therapies within the Medtronic Cardiac Rhythm Management operating unit.
Opioids associate with worse outcomes in myocardial infarction , probably because they eliminate the pain signal that informs the clinician of the urgency of revascularization. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the Crusade Quality Improvement Initiative. Do not treat AIVR.
It transforms how healthcare services are delivered, improving outcomes and optimizing resources. These advancements are utilized in specific cardiology segments, potentially enhancing patient outcomes, optimizing healthcare resources, and driving innovation in cardiac care. For instance: 1.
Rates of guideline-directed medical therapy (GDMT) prescription in real-world patients with severe heart failure (HF) with reduced ejection fraction (HFrEF), reasons for underdosing and association with outcome. Overall, ≥50% of target doses were reached in 41%, 22%, and 56% of the patients on BB, ACEi/ARB/ARNI and MRA, respectively.
Here is his ED ECG: There is bradycardia with a junctional escape. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. BP was 108 systolic (if a cuff pressure can be trusted) but appeared to be maintaining BP only by very high systemic vascular resistance. He appeared gray in color, with cool skin.
ECG#1 ECG#2 ECG#3 ECG#4 ECG#5 See outcomes of all 5 below, with the Queen of Hearts AI Bot interpretation. All of the patients presented with chest pain , and they are all in triage. Which, if any, of these patients has OMI, with myocardium at risk and need for emergent PCI? YOU TOO CAN HAVE THE PM Cardio AI BOT!!
Patient presentation is important This was a 60-something with acute chest pain: There is sinus bradycardia at a rate of 44. In case you were wondering about the T-waves and bradycardia, the K was normal. Why bradycardia? Maybe there is also inferior MI from wraparound LAD with associated sinus bradycardia.
Here is PM Cardio's Queen of Hearts interpretation (AI ECG interpretation trained by Meyers, Smith, and PM Cardio team using thousands of cases and their outcomes): The output number ranges from 0 to 1, with numbers closer to zero meaning likely NOT OMI, and numbers closer to 1 meaning OMI.
Could there have been a different outcome if the crews immediately recognized OMI – versus a shortened PR-interval – and commenced with pre-hospital Cath Lab activation? This was all very alarming because his baseline routine, otherwise, is unencumbered as he reports a usually high exertional tolerance.
Because hyperkalemia kills by either VT or VF arrest, or by bradycardia with PEA arrest, this should be assumed to be VT until proven otherwise. While the outcome is disheartening, I think this case highlights some important management principles of a fairly common cardiac arrest phenotype. Learning Points: 1.
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. The patient stabilized and had a good outcome. There is atrial fibrillation.
Case outcome The Na was 109. U waves may also be found in patients with LVH and/or bradycardia , or occasionally as a normal variant. Of course this is not a difficult case because one will always measure the K in such a case, but it does show that the K is markedly affecting cardiac electrical activity.
Triage physician interpretation: -sinus bradycardia -lateral ST depressions While there are lateral ST depressions (V5, V6) the deepest ST depressions are in V4. Ventricular fibrillation is a common outcome in OMI and should greatly heighten the suspicion for ischemic heart disease even in the absence of profound ST elevation. =
Could this outcome have been prevented with emergent cath? Like other cases on this blog who died before cath was done, I cannot prove that this patient had OMI. But I would submit to you that it is overwhelmingly likely that this was the case. I think there is a significant chance that it could have been. Were they right?
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chest pain. What do you think?
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG).
There’s sinus bradycardia, first degree AV block, normal axis, delayed R wave progression, and normal voltages. Hyperacute T waves are deflating, suggesting reperfusion but there is still reciprocal change in I/aVL and ST depression in V2, and the bradycardia is worse. Below is the ECG. What do you think? Take home 1.
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. Acute kidney injury was the most frequent possible treatment complication (515 000 per year), and bradycardia had the highest mean hospitalization costs ($17 400 [95% CI, $17 200–$17 500]).CONCLUSIONS:The
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content