This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I tell the residents: "The pacemaker is just common sense: if there is no beat, it provides one; if there is one, it keeps itself from pacing." This is similar to Ken Grauer's comment at the bottom: "What would I do if I were a pacemaker?" This made me realize that pacemaker function is not as well understood as I thought.
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Place temporary pacemaker 3. There is ventricular bigeminy with bizarre appearing wide T-waves See even more striking cases of this at the bottom of the post. The plan: 1.
My thoughts were the following: ECGs #1 and #2 showed a completely unreliable sinus pacemaker, with presumed high-grade 2nd-degree AV block — and frequent resultant pauses of over 2 seconds ( that would have been even longer had it not been for intermittent relief from the atrial escape focus ). What Does this All Mean?
Is a pacemaker needed? Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible.
There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( Some residual ischemia in the infarct border might still be present. Both episodes are initiated by an "R-on-T" phenomenon.
We admitted him for probable EP study and possible pacemaker. He underwent pacemaker placement and is doing fine. SSS is by far the most common reason for permanent pacemaker placement. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Learning Points: 1.
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. This suggests ischemia of uncertain duration. be regular! —
There are 3 etiologies I always think of with bradycardia and AV block: 1. There was no evidence of ischemia. She had a permanent pacemaker implanted. After pacer AND conversion to sinus rhythm: Computer diagnosis: IMPRESSION ELECTRONIC VENTRICULAR PACEMAKER ABNORMAL RHYTHM ECG What is missing from this interpretation?
Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. Possible mechanisms of ventricular arrhythmias elicited by ischemia followed by reperfusion. The most common triggered arrhythmia is Torsades de Pointes. Do not treat AIVR. References: Ferrier, G.
Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc).
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Poor blood supply Ischemia, or inadequate blood supply to the heart, is an abnormality that can be detected in an ECG test. ECG testing is also carried out to see how medicines work during treatment and the pacemaker's functioning.
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. He received a permanent pacemaker during the subsequent inpatient stay. Hospital transport was unremarkable.
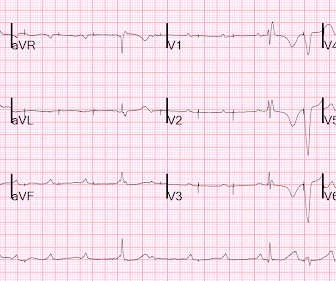
Here are inferior leads, and aVL, magnified: A closer inspection of the inferior leads and aVL Sinus bradycardia. The transvenous pacemaker was removed the following day and pressors were not required again. I had no history on the case and no prior ECG for comparison. What do you think? Peak troponin T was 3.00
Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia?
Baseline bradycardia in endurance athletes limits the use of ß-blockers. These include: i ) Use of rate-slowing medication ( ie, ß-blockers, digoxin, verapamil/diltiazem, etc. ) ; ii ) Acute or recent infarction or ischemia; iii ) Hypothyroidism; iv ) Neurologic injury; v ) Electrolyte disturbance; and , vi ) Sleep apnea.
To improve visualization — I've digitized the original ECG using PMcardio ) MY Thoughts on the ECG in Figure-1: This is a challenging tracing to interpret — because there is marked bradycardia with an irregular rhythm and a change in QRS morphology. Figure-1: The initial ECG in today's case. ( The QRS complex is wide ( ie, >0.10
Evidence of acute ischemia (may be subtle) vii. PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Left BBB vi. Pathologic Q-waves viii. LVH or RV d. Abnormal but less worrisome: i.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. It is possible there is microvascular dysfunction producing residual transmural ischemia. He told the patient this horrible news. The other point in favor of RCA is junctional rhythm.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content