This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
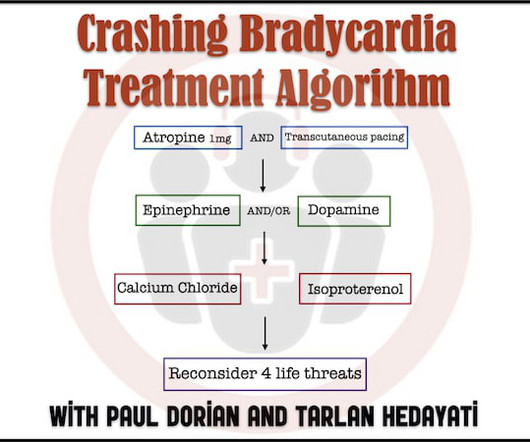
In Part 1 of our 2-part series on bradycardia and bradydysrhythmias we discussed a practical approach with electrophysiologist Paul Dorian and EM doc Tarlan Hedayati. How is the treatment of bradycardia different in the patient with hypothermia? Cardiac ischemia? In this, part 2, we discuss details of treatment. Myxedema coma?
Common explanations for unusual rhythms such as this one include: i ) Hyperkalemia ( or other severe electrolyte disorder ); ii ) Recent infarction/ischemia; iii ) Sleep apnea; iv ) Severe hypothyroidism; v ) Acute neurologic catastrophe (ie, stroke, bleed, trauma, tumor ); vi ) Some other toxicity.
No ischemia. Case continued Another ECG was recorded 3 hours later, still 1/10 pain: There is sinus bradycardia with RBBB. This is a conundrum, because it is clear that the patient is having an acute MI, the ECG is dynamic, but the pain is very mild and there is no ECG evidence of active transmural ischemia.
For instance, if there were inappropriate sinus bradycardia at less than 60 bpm, the atrial pacer would take over if it is programmed to wait 1 second before firing. The T-waves of both of these beats have, coincidentally , a superimposed P-wave Clinical course: The potassium was normal, there was no ischemia or drug toxicity.
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome.
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. There’s competing sinus bradycardia and junctional rhythm, with otherwise normal conduction, borderline right axis, normal R wave progression and voltages. What do you think?
The ECG does not show any definite signs of ischemia. IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr.
Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
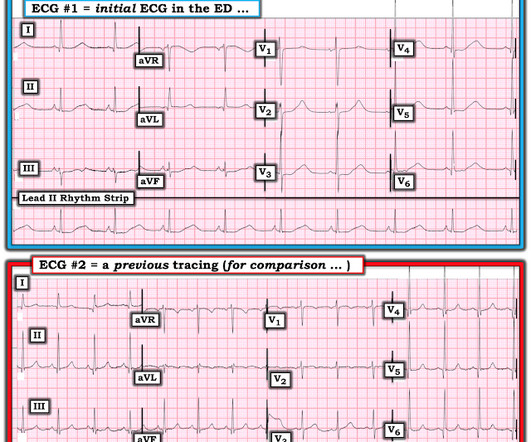
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible.
During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Acute ischemia?
The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize, and subendocardial ischemia presents with STD maximal in V5-6, II, and STE in aVR. Subendocardial ischemia does not localize.
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
Due to bradycardia, a 12-lead ECG was obtained: There is atrial fibrillation at a rate of 54. But because of bradycardia, a 12-lead was obtained, which gave the critical diagnosis. Slow atrial fibrillation implies an sick AV node, or one affected by electrolytes, ischemia, or medications/drugs. His breath alcohol was 0.259.
The patient with no prior cardiac history presented in the middle of the night with acute chest pain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. Their apparently excessive length (QT interval) is due to bradycardia. This is a case I had quite a while back.
during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Thus, there is sinus bradycardia and arrhythmia sinus pauses ( which may be longlasting, ultimately leading to sinus arrest ) and SA nodal block. The indication for pacemaker placement with SSS is symptomatic bradycardia.
Monomorphic ventricular tachycardia in the setting of acute myocardial ischemia can also be treated by intravenous lignocaine bolus followed by infusion. Predisposing causes for ventricular tachycardia like ischemia and electrolyte imbalance has to be treated simultaneously to prevent recurrence.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Chest trauma was suspected on initial exam. Here is his initial ECG around 1330: What do you think?
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). The PR and QRS intervals are both normal. ECG Blog #230 — How to compare serial ECGs.
There are 3 etiologies I always think of with bradycardia and AV block: 1. There was no evidence of ischemia. In addition to ruling out rate-slowing medication serum electrolyte disorders and/or ischemia/infarction as potential causes of bradyarrhythmias one should also rule out hypothyroidism + sleep apnea. Hyperkalemia.
Here is his previous ECG: This was my interpretation of the first ECG: Sinus bradycardia with less than 1mm ST elevation in V4-V6, elevated compared to the previous ECG, suggestive of lateral MI. This is his first ECG in the department, which I saw as it was being printed: What do you think? Notice how useful serial ECGs are!
That said — obvious findings include: i ) Marked bradycardia! — This suggests ischemia of uncertain duration. MY " Q uick T houghts" on Today's CASE: The ECG in Figure-1 is highly concerning — so it is indeed fortunate that this elderly woman came to the ED when she did! be regular! —
If you put the inferior and posterior findings together, it is diagnostic of OMI This was read as "inferior ischemia" without any other information by Dr. Richard Gray and as probable reperfused inferior-posterior OMI much later by both me and Pendell Meyers, also without any clinical information.
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. 2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. What do you think? But it is still STEMI negative.
2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia. 3] So a patient with WPW can have the pattern induced by ischemia, and there is also a report of a patient with pre-existing WPW which was “ablated” by myocardial infarction after an LAD occlusion.[4]
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. ST depression: is it ischemia? In my experience, Ive seen U waves not only with low K+/low Mg++ but also in patients with bradycardia, LVH, and sometimes in normal subjects.
Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. The patient had none of these conditions. Patient 1 remained in the hospital overnight.
There is a junctional bradycardia. Furthermore, there are T-wave changes in V2 and V3 which are highly suggestive of ischemia, but difficult to localize: anterior? Troponin was repeated and returned higher still. She was taken to the cath lab. What was the diagnosis? and right ventricular echo findings. right ventricular?
Patient presentation is important This was a 60-something with acute chest pain: There is sinus bradycardia at a rate of 44. To me, this makes the ECG nearly diagnostic of ischemia, though if it is LAD occlusion, there should be ST depression in III and aVL, so it is a bit confusing. Why bradycardia? 100% distal LAD occlusion.
Here was my answer: "Not ischemia. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. This was texted to me in real time. The patient has acute chest pain. What do you think? Maybe HOCM or another form of LVH. I would not activate cath lab.
But when the clinical presentation is sepsis, one must entertain the possibility that the ST elevation is due to demand ischemia, or some other process, and exacerbated by tachycardia. It is prudent to treat the other conditions, get the heart rate controlled, and repeat the ECG.
Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? ECG #5 — This is the 4th ECG done on the patient in this case ( obtained ~6 hours after arrival in the ED ). Use of QT-prolonging drugs?
For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. This is sinus bradycardia. More likely, these T waves probably reflect ischemia of uncertain age.
U waves may also be found in patients with LVH and/or bradycardia , or occasionally as a normal variant. This is often quite challenging to recognize — but the finding of negative U waves in a patient with chest pain is highly suggestive of ischemia ! N OTE # 1 — U waves are not specific for hypokalemia!
Here are inferior leads, and aVL, magnified: A closer inspection of the inferior leads and aVL Sinus bradycardia. I had no history on the case and no prior ECG for comparison. What do you think? The T-wave in lead III is slightly tall and broad (increased area under the curve) compared to its QRS complex.
Here is his ECG: There is no clear evidence of OMI or ischemia. The Initial ECG in Today's Case: ECG #1 showed sinus bradycardia at a rate slightly under 60/minute — normal intervals — slight left axis ( about -15 degrees ) — and no chamber enlargement. A 40-something male with no previous cardiac disease presented with chest pain.
Dr. Smith and I both ( independently ) used lead III but selection of lead aVF by the computer ( considering the bradycardia ) would yield a corrected QTc value close to the 450 msec reported. I suspect the computer in this case used lead III, or possibly lead aVF for its calculation of the QTc.
Triage physician interpretation: -sinus bradycardia -lateral ST depressions While there are lateral ST depressions (V5, V6) the deepest ST depressions are in V4. Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). 121.022866.
These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia-infarction — malignant arrhythmias — cardiac arrest — and especially Hyperkalemia. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
Baseline bradycardia in endurance athletes limits the use of ß-blockers. These include: i ) Use of rate-slowing medication ( ie, ß-blockers, digoxin, verapamil/diltiazem, etc. ) ; ii ) Acute or recent infarction or ischemia; iii ) Hypothyroidism; iv ) Neurologic injury; v ) Electrolyte disturbance; and , vi ) Sleep apnea.
The patient later settled into sinus bradycardia. He was started on amiodarone and had no more events. Next day, the cardiologists were convinced (I think correctly) that this was SVT with aberrancy that was triggered by DKA.
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
Her vital signs were within normal limits except for bradycardia at 55 bpm. It is probably sinus bradycardia with very small/depressed P-waves and prolonged PR interval. P EARL # 4 In my opinion, it is not worth wasting time trying to figure out the specific rhythm diagnosis of a bradycardia when there is hyperkalemia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content