This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
CASE CONTINUED She was admitted to the ICU. Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Smith has provided excellent overview of measuring and correcting QT interval in scenarios where QRS duration is prolonged (e.g., LBBB, ventricular pacing, etc.)." The plan: 1.
The patient stabilized and was transferred for ICU admission. Learning points: Your differential for wide QRS (by itself) and bradycardia (by itself) must include hyperkalemia. Labs resulted, showing a potassium of 8.0 mEq/L, glucose of greater than 900 mg/dL, and anion gap metabolic acidosis consistent with DKA.
His temperature was brought back to normal over time in the ICU. Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. He was extubated and had normal neurologic function.
He was admitted to the ICU and was unstable, in shock, overnight. Case Continued: He was stabilized on more calcium, pressors, and high dose insulin. 3 hours later, this was recorded at a K of 2.8 mEq/L and total calcium of 14.7 mg/dL: The massive ST Elevation persists. What is going on here?
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Syncope and Bradycardia Syncope in a 20-something woman Long QT: Do not trust the computerized QT interval when the QT is long An Alcoholic Patient with Syncope Cardiac Arrest. Is it STEMI? What is going on here?
Because hyperkalemia kills by either VT or VF arrest, or by bradycardia with PEA arrest, this should be assumed to be VT until proven otherwise. He made it to the ICU, however the patient unfortunately expired approximately 24 hours after ICU admission. We set the machine to synchronized cardioversion.
He was admitted to the ICU and transferred emergently to a facility where he could undergo emergent dialysis as a part of further evaluation and management. ST elevation in aVL with reciprocal ST depression in the inferior leads Shock, bradycardia, ST Elevation in V1 and V2. The QRS is narrow and T waves are much less peaked.
Upon arrival in the ICU, before getting Continuous Veno-Venous Hemodialysis (CVVHD), his potassium had risen again to 7.8 Hyperkalemia findings include the classic peaked T-waves, as well as the deadly B's of hyperkalemia: Broad (wide QRS), Brady (bradycardia), Blocks (AV blocks), and Bizarre. There is no ECG available from this time.
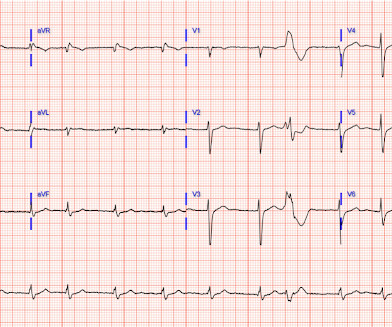
Theres sinus bradycardia, borderline PR interval, narrow QRS; normal axis/R wave progression; low precordial voltages, and subtle peaked T waves (most obvious in V2, but all T waves are symmetric with a narrow base). Theres no prior ECG to compare - but the bradycardia, prolonged PR and peaked T waves could all be from hyperkalemia.
She was resuscitated and admitted to ICU for presumed sepsis. Several days into hospitalization, she continued to have occasional episodes of sinus rhythm and sinus bradycardia with periods of Mobitz I AV block and 2:1 block. Meanwhile, the patient's native rhythm is sinus bradycardia with adequate perfusion.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content