This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Electrocardiogram (ECG) and telemetry revealed junctional bradycardia with heart rate in 30s and sinus pauses (5-7 seconds). He was admitted for further workup of bradycardia. His home medications included metoprolol succinate 25mg daily which was held given bradycardia. Initial laboratory analysis was unremarkable.
A recently opened clinical trial called BACKBEAT (BradycArdia paCemaKer for Blood prEssure treAtmenT) aims to use Medtronic’s Astra and Azure model pacemakers to not only treat slow heart rates but also delivers electrical pulses stimulating the heart in a way that reduces the patient’s blood pressure.
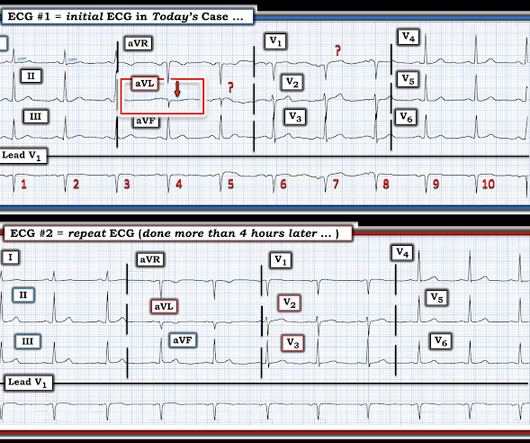
He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder. IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr.
Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical. Risk Reduction Data from wearables can identify potential risks, such as undiagnosed arrhythmias or hypertension, allowing healthcare teams to address these issues before surgery.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chest pain and diaphoresis. preceding each of the fascicular beats — indicating a faster rate for the escape rhythm compared to the sinus bradycardia ).
Q waves in association with RBBB are usually not seen in anterior leads unless there is pulmonary hypertension or anterior infarction. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury.
A 56 year old male with PMHx significant for hypertension had chest pain for several hours, then presented to the ED in the middle of the night. Case continued Another ECG was recorded 3 hours later, still 1/10 pain: There is sinus bradycardia with RBBB. The pain was located in the mid to left chest and developed after riding his bike.
A middle-aged woman with a history of hypertension presented with typical chest pain. Her BP was 160/80. Here was her presenting ECG, with chest pain: Inferior leads show hyperacute T-waves and reciprocal STD in aVL, with a reciprocally hyperacute T-wave in aVL. This is all but diagnostic of inferior OMI. There is also subtle STE in V1-V3.
For participants who slept just 5 hours per night, hypertension risk increased by 29%, depression risk increased by 64%, and anxiety risk increased by 46%. One last important finding regarding sleep duration was the J-shaped association between nightly sleep duration and the risk of hypertension, anxiety, and depression.
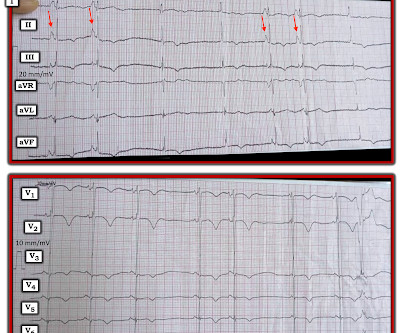
Perhaps the patient has pulmonary hypertension and/or tricuspid regurgitation? There definitel are periods of bradycardia (so pacing may be needed for that). Hope this helps — :) ECG-3 — I see sinus bradycardia and arrhythmia. RED arrows show what looks to be sinus P waves that are HUGE !!!!
A few days later, midodrine and fludrocortisone were held due to hypertension and the patient was discharged. This is supported by the PT note which described a palpably irregular pulse with pauses and marked bradycardia. Cardiology was consulted, and the note said "no arrhythmias on telemetry or pacer interrogation."
Vital signs were noted to be unremarkable with respect to any hypo-hypertensive crisis, hypoxia, etc. He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Fire/EMS crews found him clammy and uncomfortable.
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction. This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech.
Tricuspid regurgitation jet velocity and pulmonary regurgitation end diastolic velocity indicating pulmonary hypertension are also taken as surrogates of left atrial pressure in the absence of pulmonary disease. Use of drugs producing bradycardia like beta blockers in stages III and IV may precipitate low output state.
The BACKBEAT pivotal study will evaluate the efficacy and safety of atrioventricular interval modulation (“AVIM”) therapy (also known as BackBeat CNT), for the treatment of pacemaker-indicated patients with uncontrolled hypertension despite the use of antihypertensive medications. Orchestra BioMed and Medtronic, Inc. Kowal, M.D., Kowal, M.D.,
Does this patient have hypertension and/or heart failure that has worsened? In my experience, Ive seen U waves not only with low K+/low Mg++ but also in patients with bradycardia, LVH, and sometimes in normal subjects. NOTE: We do not know how long ago this baseline tracing was done!
Initial vitals show hypertension (175/85), Atrial Fibrillation with RVR as seen in Figure 1 , hypercapnia (99mmHg), and SPO2 of 100%. Crew notifies the received ED of an incoming post-arrest patient and notes a sinus bradycardia on their monitor, as seen in Figure 2. Epinephrine administered intravenously.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ). The syncope lasted about 2-3 minutes according to his wife.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. MY Thoughts on the ECG in Figure-1: The rhythm in ECG #1 is sinus bradycardia at ~50-55/minute. It is unknown when this pain recurred and became constant.
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. The corrected QT interval is extremely long, about 500 ms.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. Here is his triage ECG which was obtained at 20:34 during active pain.
Written by Jesse McLaren An 80 year old patient with diabetes/hypertension/ cirrhosis had a recent increase in candesartan for their hypertension, and was also on spirolactone and nadolol. Theres no prior ECG to compare - but the bradycardia, prolonged PR and peaked T waves could all be from hyperkalemia. Take away 1.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. A post-cath EKG was recorded at 0719: The computer interpretation read Sinus bradycardia, otherwise normal ECG. The troponin peaked at 0.4
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content