This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
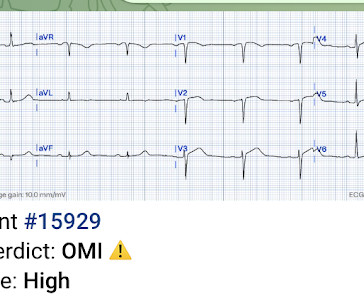
There’s competing sinus bradycardia and junctional rhythm, with otherwise normal conduction, borderline right axis, normal R wave progression and voltages. While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky.
There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. The cardiologists were not familiar with this and insisted that the ECG in paced rhythm could not be used to "look for a STEMI".
He has now implemented the Queen of Hearts in his hospital. The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. This case was sent by Dr. Jean-christophe Reiters, an interventionalist in Belgium. He has been following the blog for 4 years. He wanted to share one of the first cases.
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ).
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. Patient 1 remained in the hospital overnight.
It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Could there have been a different outcome if the crews immediately recognized OMI – versus a shortened PR-interval – and commenced with pre-hospital Cath Lab activation? Is this OMI?
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. Why bradycardia? QTc is the computer measurement.
This was sent to me by a former resident from a community hospital: A middle-aged woman complained of chest pain and was seen in triage. The computer interpreted the ECG (GE Marquette 12 SL) as: "Sinus Bradycardia. Here it is: Computer interpretation: "Sinus bradycardia. She had a ECG recorded. Normal ECG."
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI.
Triage physician interpretation: -sinus bradycardia -lateral ST depressions While there are lateral ST depressions (V5, V6) the deepest ST depressions are in V4. The patient was started on dual antiplatelet therapy and discharged from the hospital on day 3 without further event. Triage EKG: What do you think?
There’s sinus bradycardia, normal conduction, normal axis, delayed R wave progression, and normal voltages. The patient has a history of CABG so some of these changes could be old, but with ongoing chest pain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. Sinus bradycardia.”
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. EKG is pictured below: What do you think?
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Learning Points: 1.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient was extubated on Day-3 of the hospital stay. The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. The below ECG was recorded.
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Is it STEMI? Syncope and Bradycardia Syncope in a 20-something woman Long QT: Do not trust the computerized QT interval when the QT is long An Alcoholic Patient with Syncope Cardiac Arrest.
The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chest pain. The whole paradigm is literally called "STEMI" vs. "NSTEMI." Canto et al.
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". A few days later an ECG was repeated which showed normal sinus rhythm with no further hyperkalemia findings: After a 3-week hospitalization for acute renal failure, hyperkalemia, and compartment syndrome, the patient was discharged to acute rehab.
They presented to a hospital clinic for routine paracentesis, after which they developed nausea and syncope attributed to a vasovagal episode from the procedure. Theres no prior ECG to compare - but the bradycardia, prolonged PR and peaked T waves could all be from hyperkalemia. Labs showed a non-hemolyzed potassium of 6.2,
Despite the baseline artifact theres sinus bradycardia, convex ST elevation in III, reciprocal ST depression in aVL and possible anterior ST depression indicating inferoposterior OMI. STEMI criteria are only 43% sensitive for OMI. Beware confusing the diagnosis of posterior STEMI by using posterior leads.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content