This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Methods Consecutive patients with bradycardia indicated for pacing from 2016 to 2022 were prospectively followed for the clinical endpoints of heart failure (HF)-hospitalizations and all-cause mortality at 2 years. 6.60) were associated with increased hazard of HF-hospitalizations, and RVP (2.52, 95% CI: 1.19–5.35)
The implantation of leadless pacemakers has grown in recent years for the management of bradycardias. There are no randomized controlled trials to evaluate outcomes for single-chamber transvenous (TV), dual-chamber TV, and leadless pacemakers.
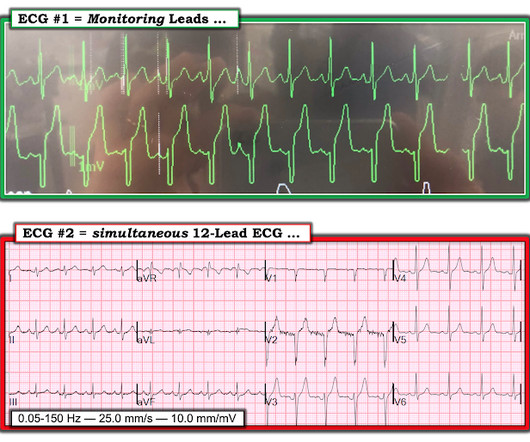
Written by Willy Frick A man in his 70s with a history of HFrEF and sick sinus syndrome s/p dual chamber pacemaker placement was admitted for overnight observation following outpatient placement of a mitral valve clip. This is unambiguous evidence of pacemaker malfunction. Imagine the pacemaker is set at a minimum rate of 60.
Introduction: Leadless pacemakers (LP) are increasingly utilized in pts with bradycardia and may be associated with better outcomes compared to right ventricular pacing (RVP). Conduction system pacing (CSP) with HBP or LBBAP have been associated with reduction in death or heart failure hospitalization (HFH).
Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. She was intubated and a transvenous pacemaker was inserted with good capture. In addition to marked bradycardia — could there be high-grade AV block? Atropine produced no response. She received PR aspirin.
A newborn male was delivered via cesarean section at term due to acute fetal distress and fetal bradycardia, necessitating emergency pacemaker implantation. During hospitalization, the infant experienced multiple seizures and episodes of hypoglycemia.
The patient was extubated on Day-3 of the hospital stay. The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ).
For full discussion of the case — CLICK HERE — ECG Rhythm Overview: A 12-year-old boy was admitted to our hospital with severe myocardial dysfunction and chaotic rhythm with tachy- and bradycardic arrhythmias. ECG #2: Figure-2: ECG #2 is from the 4th hospital day. In the meantime, a pacemaker may be needed. =
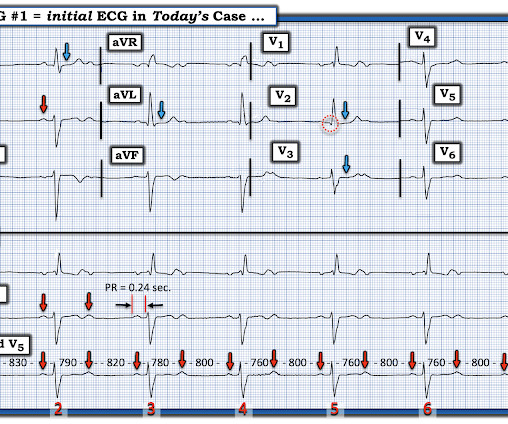
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study. be regular! —
Conclusions This study is expected to provide valuable findings regarding arrhythmia in HFnon-rEF patients, and elucidate a potential new therapeutic approach for HFnon-rEF.
There are 3 etiologies I always think of with bradycardia and AV block: 1. She had a permanent pacemaker implanted. After pacer AND conversion to sinus rhythm: Computer diagnosis: IMPRESSION ELECTRONIC VENTRICULAR PACEMAKER ABNORMAL RHYTHM ECG What is missing from this interpretation? Hyperkalemia. Her K was normal 3.
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
Hospital transport was unremarkable. He received a permanent pacemaker during the subsequent inpatient stay. plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia.
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Because of its potential for invoking uneeded cardiac catheterization or hospital admission — it is worth periodically reviewing this ECG pattern.
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
Written by Willy Frick A woman in her 70s is hospitalized with undifferentiated shock after being found down at home. Several days into hospitalization, she continued to have occasional episodes of sinus rhythm and sinus bradycardia with periods of Mobitz I AV block and 2:1 block. Here is her cardiac telemetry.
The patient went for EP study and had prolonged HV interval which strongly supports placement of a pacemaker. He underwent dual chamber pacemaker implantation and did well. Quite surprisingly, carotid massage slows the sinus rate slightly, and as a result instantly improves AV conduction to 1:1, supporting Mobitz II AV block!
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content