This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
How do we figure out when bradycardia is due to a medical illness and when it is a primary cardiac problem? The post Ep 154: 4-Step Approach to Bradycardia and Bradydysrhythmias appeared first on Emergency Medicine Cases. What are some key ECG patterns that are sometimes missed by ED docs that can have devastating consequences?
Electrocardiogram (ECG) and telemetry revealed junctional bradycardia with heart rate in 30s and sinus pauses (5-7 seconds). He was admitted for further workup of bradycardia. His home medications included metoprolol succinate 25mg daily which was held given bradycardia. Initial laboratory analysis was unremarkable.
In-hospital cardiac arrest (IHCA) is a major healthcare problem with a high mortality rate. With continuous telemetry monitoring, heart rate trends could be used to predict IHCA events.
Methods Consecutive patients with bradycardia indicated for pacing from 2016 to 2022 were prospectively followed for the clinical endpoints of heart failure (HF)-hospitalizations and all-cause mortality at 2 years. 6.60) were associated with increased hazard of HF-hospitalizations, and RVP (2.52, 95% CI: 1.19–5.35)
Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. In addition to marked bradycardia — could there be high-grade AV block? On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic.
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
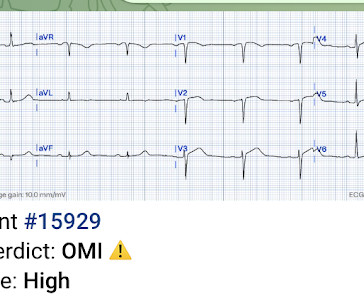
He has now implemented the Queen of Hearts in his hospital. The app also states that there is "suspected" ACS without ST elevation (NSTEMI), posterior fascicular block, sinus bradycardia, and LVH) Note on version 1 of the Queen: she will diagnose "OMI" whether it is an active or reperfused OMI.
The primary outcome was ventricular arrhythmias, the secondary outcomes were bradycardia and atrial fibrillation (AF).ResultsOur Perioperative or postoperative use of DEX reduced the incidence of in-hospital ventricular arrhythmias [Odds Ratio (OR) 0.14, 95% Confidence Interval (CI) 0.03–0.66], 8.17) compared with propofol.
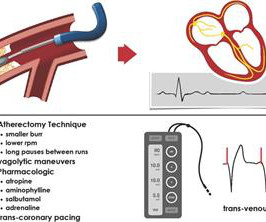
Background Rotational atherectomy (RA) during percutaneous coronary intervention may cause transient bradycardia or a higher-degree heart block. Traditionally, some operators use prophylactic transvenous pacing wire (TPW) to avoid haemodynamic complications associated with bradycardia. No patients underwent prophylactic TPW insertion.
There’s competing sinus bradycardia and junctional rhythm, with otherwise normal conduction, borderline right axis, normal R wave progression and voltages. Significant bradycardia ( rate in the 40s/minute ) — is present throughout. What do you think? It’s unclear if the paramedic ECGs were seen or missed in the ED.
The implantation of leadless pacemakers has grown in recent years for the management of bradycardias. There are no randomized controlled trials to evaluate outcomes for single-chamber transvenous (TV), dual-chamber TV, and leadless pacemakers.
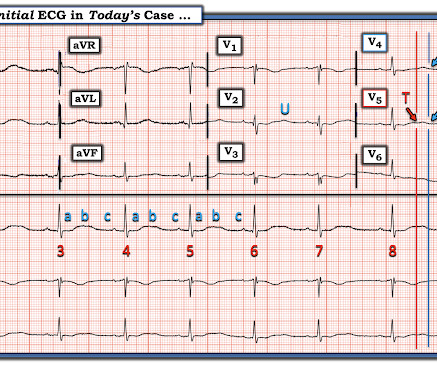
This ECG shows sinus bradycardia with massively long QT (or QU?) Especially when present in the setting of bradycardia and syncopal episodes, this is very worrisome for high risk of lethal dysrhythmias including polymorphic ventricular fibrillation (termed Torsades when in the setting of long QT). interval, at over 600 msec.
The patient was extubated on Day-3 of the hospital stay. The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ).
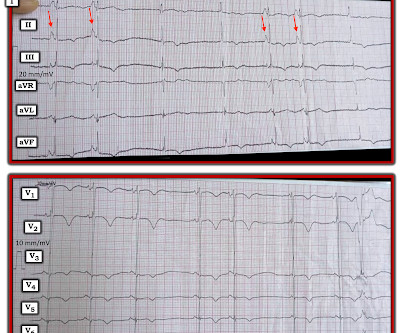
He was hospitalized one week prior to EMS arrival for a seizure with no other recent illnesses or injuries. Bradycardia with “borderline hypotension” as described by the paramedics (BP 104/40) with 3-lead ECG as seen in Figure 1 were found. BVM was continued via NPA and the patient transported to the closest hospital.
A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. She is healthy with no known cardiac disease. She was admitted to the neurology department due to headache and vomiting.
Introduction: Leadless pacemakers (LP) are increasingly utilized in pts with bradycardia and may be associated with better outcomes compared to right ventricular pacing (RVP). Conduction system pacing (CSP) with HBP or LBBAP have been associated with reduction in death or heart failure hospitalization (HFH).
A newborn male was delivered via cesarean section at term due to acute fetal distress and fetal bradycardia, necessitating emergency pacemaker implantation. During hospitalization, the infant experienced multiple seizures and episodes of hypoglycemia.
For full discussion of the case — CLICK HERE — ECG Rhythm Overview: A 12-year-old boy was admitted to our hospital with severe myocardial dysfunction and chaotic rhythm with tachy- and bradycardic arrhythmias. ECG #2: Figure-2: ECG #2 is from the 4th hospital day. Hope this helps — :) ECG-3 — I see sinus bradycardia and arrhythmia.
Between 81-95% of life-threatening ventricular dysrhythmias and acute cardiac failure occur within 24-48 hours of hospitalization. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury.
Methods The TriNetX database (Jan 2015June 2023) was queried to include adults receiving their first single-chamber ventricular pacemaker for heart block, bradycardia, sick sinus syndrome, atrial fibrillation, or syncope, excluding those with prior pacemakers, heart failure or enrolled for research settings. were males, with mean ages of 74.9
The patient and his wife suspected this was due to withholding of his midodrine and fludrocortisone during the hospitalization for his procedure. A few days after that, he was hospitalized for an unrelated reason, an abdominal infection. On the day of hospitalization, he had a CT scan. The case continues.
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Syncope and Bradycardia Syncope in a 20-something woman Long QT: Do not trust the computerized QT interval when the QT is long An Alcoholic Patient with Syncope Cardiac Arrest. Is it STEMI? What is going on here?
Secondary endpoints are 30 s or more persistent supraventricular tachycardia and ventricular tachycardia, 3 s or more persistent pause, bradycardia with 40 beats per minutes or lower heart rate, AF burden, all-cause death, cardiovascular death, hospital readmission due to exacerbation of HF, acute coronary syndrome, ischaemic or haemorrhagic stroke, (..)
He was later transferred back to his local hospital neurologically intact and without serious sequela. See this case and this case for more examples of ACS involving the LMCA Learning points: LMCA occlusion carries a poor prognosis, most patients do not make it to the hospital. Long term follow up is not available.
Lower panels: Kaplan–Meier curves for 1-year all-cause death or HF hospitalization according to beta-blockers, ACEi/ARB/ARNI and MRA prescription and dosing. Treatment with BB and ACEi/ARB/ARNI were associated with a lower risk of death or HF hospitalizations (adjusted hazard ratio [HR] 0.63, 95% confidence interval [CI] 0.48–0.84,
This was sent to me by a former resident from a community hospital: A middle-aged woman complained of chest pain and was seen in triage. The computer interpreted the ECG (GE Marquette 12 SL) as: "Sinus Bradycardia. Here it is: Computer interpretation: "Sinus bradycardia. She had a ECG recorded. Normal ECG."
The rule of thumb is less accurate, and the risk is higher because a long QT in the presence of bradycardia ("pause dependent" Torsades) predisposes to Torsades. 6) Use a different rule of thumb for bradycardia : Manually approximate both the QT and the RR interval. 3) At heart rates below 60, far more caution is due.
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study. be regular! —
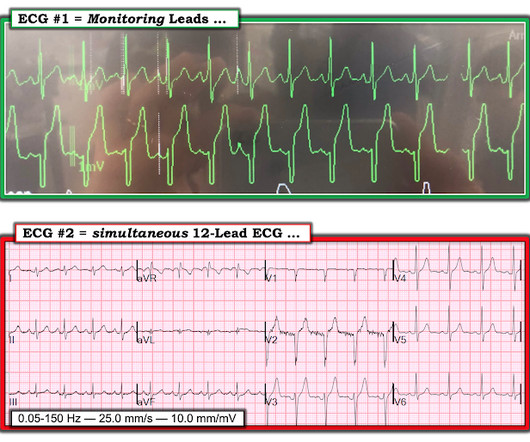
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. About 20 minutes later ( on the way to the hospital ) — the patient's CP resolved, and ECG #1 was recorded. That said, even without more history and without a prior ECG for comparison — the initial ECG in Figure-1 clearly is of concern!
The relationship between low RHR and CI has yet to be described.Purpose:We hypothesize that resting sinus bradycardia (low RHR) could be a predictor of chronotropic incompetence and reduced exercise capacity.Methods:The derivation cohort consists of 201 patients with normal Bruce protocol treadmill stress echocardiogram.
A few days later an ECG was repeated which showed normal sinus rhythm with no further hyperkalemia findings: After a 3-week hospitalization for acute renal failure, hyperkalemia, and compartment syndrome, the patient was discharged to acute rehab. He went emergently to the OR for fasciotomy due to compartment syndrome. With a twist.
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. Recently, hospitals have failed to identify 25% of cases of cardiac arrest. The profound learning provides phenotyping of cardiovascular health in seconds.
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. The corrected QT interval is extremely long, about 500 ms. However, the mean level (2.50.4
There are 3 etiologies I always think of with bradycardia and AV block: 1. While the diagnosis of SSS may become readily apparent early on in many patients clear indication for pacing usually does not become established until there is profound, symptomatic bradycardia usually requiring pauses of at least 3.0 Hyperkalemia.
Patient 1 remained in the hospital overnight. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. Angiography revealed a 30% nonobstructive stenosis of the mid LAD. Serial high sensitivity troponin T (URL 15 ng/L) values were negative and stagnant. He went to the cath lab at 0900 the next morning.
Hospital transport was unremarkable. plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. The patient advised overall improvement with complete resolution of symptoms.
Could there have been a different outcome if the crews immediately recognized OMI – versus a shortened PR-interval – and commenced with pre-hospital Cath Lab activation? This was all very alarming because his baseline routine, otherwise, is unencumbered as he reports a usually high exertional tolerance.
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Because of its potential for invoking uneeded cardiac catheterization or hospital admission — it is worth periodically reviewing this ECG pattern.
Case 4 Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 Patient presentation is important This was a 60-something with acute chest pain: There is sinus bradycardia at a rate of 44. In case you were wondering about the T-waves and bradycardia, the K was normal. Why bradycardia?
C HALLENGE : Take another LOOK at the first 2 tracings shown in today's case. For clarity in Figure-1 — I've reproduced and put these first 2 ECGs together. Laddergram Illustration: The mechanism of AV block in ECG #2 is complex.
Written by Pendell Meyers We received a call from an outside hospital asking to transfer a "traumatic post arrest" patient. Hyperkalemia findings include the classic peaked T-waves, as well as the deadly B's of hyperkalemia: Broad (wide QRS), Brady (bradycardia), Blocks (AV blocks), and Bizarre.
We have countless cases of missed posterior MI on this blog, including these: Interventionalist at the Receiving Hospital: "No STEMI, no cath. I do not accept the transfer." "It It isn't a STEMI," so cath lab refusal (again). Were they right?
Triage physician interpretation: -sinus bradycardia -lateral ST depressions While there are lateral ST depressions (V5, V6) the deepest ST depressions are in V4. The patient was started on dual antiplatelet therapy and discharged from the hospital on day 3 without further event. Triage EKG: What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content