This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Methods Consecutive patients with bradycardia indicated for pacing from 2016 to 2022 were prospectively followed for the clinical endpoints of heart failure (HF)-hospitalizations and all-cause mortality at 2 years. CSP should be preferred over VSP or RVP during pacing for bradycardia.
ABSTRACT Background Despite leadless pacemakers (LPMs) showing promise, real-world data comparing them to transvenous pacemakers (TV-VVI) are insufficient and often contradictory, especially in patients without major comorbidities like heart failure. Objectives Comparing LPMs with TV-VVIs in real-world patients without HF.
LP, leadless pacemaker; PCT, pacing capture threshold; AUC, area under the curve. ABSTRACT Introduction Leadless pacemakers (LPs) are a valuable treatment for bradycardia, with the Aveir offering advanced features, including a protective sleeve and active fixation.
Methods Thirty-seven patients with a pacemaker indication for bradycardia or cardiac resynchronization therapy underwent LBBAP implantation. ECG, vectorcardiogram, ECG belt and UHF-ECG signals were recorded during RVP, LVSP and LBBP, and intrinsic activation.
Complete left bundle branch block (CLBBB)-like QRS morphology of right ventricular pacing at pacemaker implantation satisfying the American Heart Association/American College of Cardiology Foundation/Heart Rhythm Society criteria of CLBBB was associated with development of pacing induced cardiomyopathy.
Abstract Introduction Severe transitory episodes of bradycardia with subsequent syncope in children are common, and generally portend a benign prognosis. Conclusion CNA may be an effective alternative to pacemaker implantation in pediatric patients with syncope or significant symptoms secondary to functional SP or AVB. s (range 0.8–2.2)
He received a permanent pacemaker during the subsequent inpatient stay. plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. Hospital transport was unremarkable. 7] Callans, D.
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
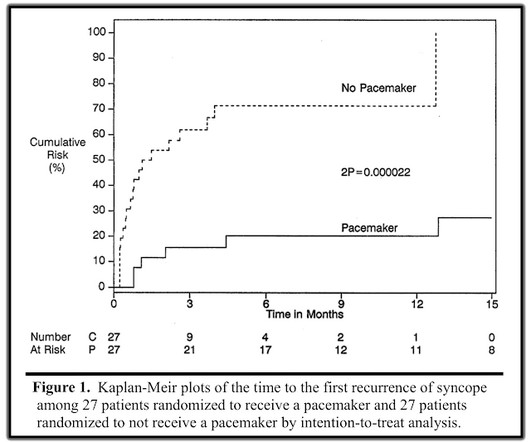
He was discharged with an event monitor and electrophysiology follow up. If the block is not vagal in nature, the patient should receive a pacemaker. There was a randomized trial to determine whether pacemakers could benefit patients with vasovagal syncope, aptly named The North American Vasovagal Pacemaker Study (VPS).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content