This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct. Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias.
Methods Consecutive patients with bradycardia indicated for pacing from 2016 to 2022 were prospectively followed for the clinical endpoints of heart failure (HF)-hospitalizations and all-cause mortality at 2 years. CSP should be preferred over VSP or RVP during pacing for bradycardia.
Procedure and fluoroscopy time, pacing parameters, electrophysiological and echocardiographic characteristics, as well as complications were recorded at implantation and during follow-up. Methods This is a single-center, prospective, randomized controlled study. min, p = .002). Conclusion TTE-guided LBBP is a feasible and safe method.
Methods Thirty-seven patients with a pacemaker indication for bradycardia or cardiac resynchronization therapy underwent LBBAP implantation. ECG, vectorcardiogram, ECG belt and UHF-ECG signals were recorded during RVP, LVSP and LBBP, and intrinsic activation.
Bradycardia with “borderline hypotension” as described by the paramedics (BP 104/40) with 3-lead ECG as seen in Figure 1 were found. Paramedics note that he is only responsive to deep painful stimuli with shallow ventilations. Rhonchi are auscultated bilaterally. Figure 1: Paramedics correctly note that this is a Complete Heart Block.
Chronic recurrent monomorphic VT like fascicular tachycardia and right ventricular outflow tract tachycardia are also amenable to electrophysiological mapping and ablation. Monitor screen shot showing ventricular tachycardia and restoration of sinus rhythm following cardioversion with a direct current shock.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Serious AEs were rare; 1 patient in the etripamil arm experienced transient severe bradycardia and syncope, assessed as due to hyper-vagotonia.Conclusions:Intranasal etripamil 70 mg reduced VR and improved symptom-relief and treatment-satisfaction.
Methods The TriNetX database (Jan 2015June 2023) was queried to include adults receiving their first single-chamber ventricular pacemaker for heart block, bradycardia, sick sinus syndrome, atrial fibrillation, or syncope, excluding those with prior pacemakers, heart failure or enrolled for research settings.
ABSTRACT Introduction Leadless pacemakers (LPs) are a valuable treatment for bradycardia, with the Aveir offering advanced features, including a protective sleeve and active fixation. The higher impedance during the implantation was a strong predictor of a midterm favorable PCT.
Abstract Introduction Severe transitory episodes of bradycardia with subsequent syncope in children are common, and generally portend a benign prognosis. Rarely, patients may experience prolonged asystolic episodes secondary to significant sinus pauses (SP) or paroxysmal atrioventricular block (AVB).
Patients who received pacemakers for an advanced atrioventricular block or bradycardia with atrial fibrillation, baseline LV ejection fraction (LVEF) ≥ 50%, and echocardiogram recorded at least 6 months postimplantation were included. The paced QRS recorded immediately after implantation was analyzed.
years during which 14 patients (18%) experienced VA requiring treatment ( n = 14) or syncope due to bradycardia ( n = 2). Patients were followed for 1.6 ± 1.5 Four/9 patients (44%) with MVP experienced VA ( n = 3) or syncope ( n = 1). 95% confidence interval: [1.2–27], 27], p = 0.03, log-rank p = 0.03).
2 weeks Here is the final electrophysiology note: It is unclear what precipitated his motor vehicle collision. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Sinus Tachycardia ( common in any trauma patient. ).
plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. Josephson’s Clinical Cardiac Electrophysiology: Techniques and Interpretations (6th ed). Phase IV block, or concealed transeptal conduction).
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. The corrected QT interval is extremely long, about 500 ms.
She has not yet been seen by electrophysiology or had further genetic testing for Brugada syndrome. As for our patient, on discharge, her EKG had completed returned to her baseline morphology and she has been doing well in follow-up.
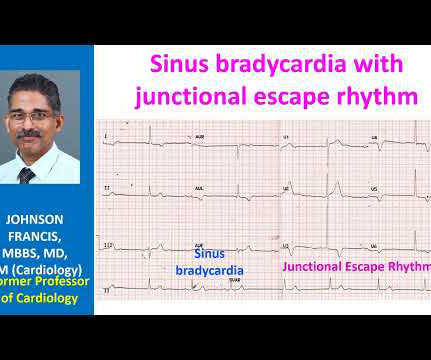
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
Patient 2 : 55 year old with 5 hours of chest pain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Smith : The fact that the ECG did not evolve is further proof that this was the baseline ECG. nearly identical to the first case).
may influence cardiac electrophysiology and the susceptibility to cardiac arrhythmias. as a potential therapeutic target for bradycardia-dependent arrhythmias. BackgroundPrevious studies suggested that SCN10A/Nav1.8 Notably, the expression of SCN10A is not uniform, showing variable expression in each cardiac chamber.
Regardless of further evaluation, she should avoid bradycardia, AV nodal blockers, Na channel blockers, and fevers. --If A score including ECG pattern, early familial SCD antecedents, inducible electrophysiological study, presentation as syncope or as aborted SCD and SND had a predictive performance of 0.82.
The most common indications for S-ICD extraction were the need for bradycardia pacing (frequency among extractions, 18.2%), infection (22.7%), and inappropriate shocks due to oversensing (22.7%). There were 22 (5.9%) patients (81.8% male; 52.1 ± 13.2 years old) who underwent S-ICD extraction over a median follow-up period of 4.4 [2.0−6.5]
He was discharged with an event monitor and electrophysiology follow up. Perhaps because the bradycardia in vasovagal syncope is only one part of the autonomic response. Phase 4 block is also referred to as "bradycardia dependent block." He subsequently woke up on the ground, unsure how long he had been unconscious.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content