This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome.
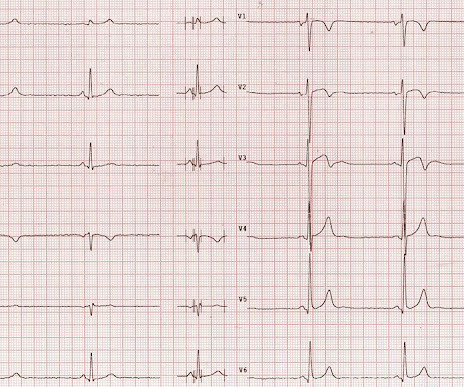
Description Sinus bradycardia. There is ST elevation in V2 and V3 There are inverted T-waves in V2 and V3 There are prominent U-waves in V2 and V3 Many responders were worried about ischemia or hypertrophic cardiomyopathy. This short QT at least makes ischemia all but impossible. There is high voltage. This is a normal variant.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Hopefully a repeat echocardiogram will be performed outpatient. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Chest trauma was suspected on initial exam.
Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. The patient had none of these conditions.
Soon afterward, the patient’s symptoms return along with lightheadedness, bradycardia, and hypotension. The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. The Queen of Hearts agrees: Around this time his initial high sensitivity troponin I resulted at 231 ng/L.
However, an echocardiogram is a different test, also conducted for heart activity. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiac arrest. ECG and EKG refer to the same thing.
If you put the inferior and posterior findings together, it is diagnostic of OMI This was read as "inferior ischemia" without any other information by Dr. Richard Gray and as probable reperfused inferior-posterior OMI much later by both me and Pendell Meyers, also without any clinical information.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab.
An echocardiogram was done. These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia-infarction — malignant arrhythmias — cardiac arrest — and especially Hyperkalemia. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
Evidence of acute ischemia (may be subtle) vii. PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Left BBB vi. Pathologic Q-waves viii. LVH or RV d. Abnormal but less worrisome: i.
That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. Below in Figure-5 is a 10-minute continuous lead II recording on oral Flecainide, now showing sinus bradycardia without a single PVC! It is reasonable to perform an echocardiogram to evaluate LV function. He has since been free of PVCs.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content