This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
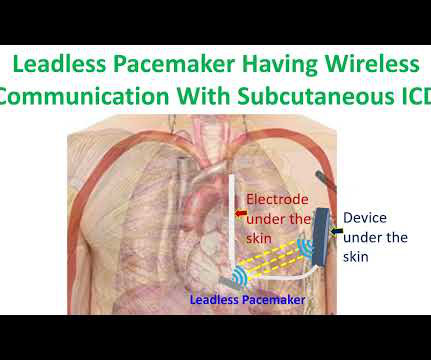
(MedPage Today) -- BOSTON -- A leadless pacemaker reliably communicated with a subcutaneous implantable cardioverter-defibrillator (S-ICD) to deliver anti-tachycardia (ATP) and bradycardia pacing, the MODULAR ATP study showed. In terms of safety.
Is a novel modular pacing–defibrillator system, consisting of a leadless pacemaker in wireless communication with a subcutaneous implantable cardioverter–defibrillator (ICD), able to effectively and safely provide antitachycardia and bradycardia pacing?
The following are key points to remember from a review article on cardiac implantable electronic devices (CIEDs), which include pacemakers for bradycardia, biventricular pacemakers for heart failure, and implantable cardioverter–defibrillators (ICDs) for the treatment of sudden cardiac death:
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Place temporary pacemaker 3. There is ventricular bigeminy with bizarre appearing wide T-waves See even more striking cases of this at the bottom of the post. The plan: 1. No wall motion abnormality.
This is demonstrated ( Figure 5 ) by the gap in arrows at the bottom of the strip, signifying that the demand pacemaker has recognized an underlying rhythm (in this case, artifact from a moving ambulance). The artifact fools the pacemaker into thinking the rhythm is native.
He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. Some episodes of PMVT would terminate spontaneously — but on many occasions, the PMVT degenerated to VFib, requiring defibrillation.
Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). The above ECG initially shows AV block. A run of very fast, irregular polymorphic VT ensues.
She was never defibrillated. Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. As was seen in this case — defibrillation and/or overdrive pacing may be needed. What do you think?
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion.
Subcutaneous implantable cardioverter defibrillator was an innovation meant to reduce the lead related problems of conventional transvenous ICDs. But subcutaneous ICD cannot provide bradycardia and antitachycardia pacing as a transvenous ICD. of patients were free from leadless pacemaker related major complications. 2024 May 18.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. 2:34 PM, following right heart catheterization She then went into atrial fibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content