This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- BOSTON -- A leadless pacemaker reliably communicated with a subcutaneous implantable cardioverter-defibrillator (S-ICD) to deliver anti-tachycardia (ATP) and bradycardia pacing, the MODULAR ATP study showed. In terms of safety.
Wireless implantable cardioverter-defibrillators (ICDs) eliminate the lead-related complications that come with a wired ICD, but they are unsuitable for patients with ventricular tachycardia, when the heart beats too quickly, or bradycardia, when the resting heart rate is seen as low.
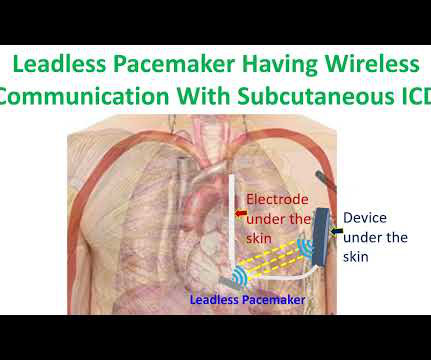
Is a novel modular pacing–defibrillator system, consisting of a leadless pacemaker in wireless communication with a subcutaneous implantable cardioverter–defibrillator (ICD), able to effectively and safely provide antitachycardia and bradycardia pacing?
Here is the transcript of the video: Implantable defibrillator is an important life saving device. Then, why is it mentioned that, implanting a defibrillator soon after an acute myocardial infarction, in those with left ventricular dysfunction and prone for ventricular arrhythmias and sudden cardiac death, is not useful?
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction. The plan: 1.
He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. Some episodes of PMVT would terminate spontaneously — but on many occasions, the PMVT degenerated to VFib, requiring defibrillation.
The following are key points to remember from a review article on cardiac implantable electronic devices (CIEDs), which include pacemakers for bradycardia, biventricular pacemakers for heart failure, and implantable cardioverter–defibrillators (ICDs) for the treatment of sudden cardiac death:
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. There is sinus bradycardia with one PVC. An elderly woman had sudden ventricular fibrillation. The K was normal.
VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Then the patient would have been taken to the critical care area with a defibrillator at his side while waiting for the cath lab to be ready. MY Thoughts on the ECG in Figure-1: The rhythm in ECG #1 is sinus bradycardia at ~50-55/minute.
Recurrent ventricular tachycardia in spite of radiofrequency catheter ablation needs an implantable cardioverter defibrillator. Those at risk of recurrent VT with previous myocardial infarction and left ventricular dysfunction also need an implantable defibrillator.
During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. She spontaneously converted (Defibrillation was not performed). This is what T-waves look like when there is a long QT."
Learning points: TCP is primarily recommended for bradycardia that does not respond to atropine, or other agents. As this case shows, electrical capture isn't always possible at lower currents, especially with pads placed in a standard anterolateral "defibrillation" position.
The arrhythmia spontaneously converted before defibrillation was achieved. As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ). Just prior to arrival he fell out of consciousness with the below ECG on the monitor.
EMS report was that the patient had unknown down time with unwitnessed arrest, found initially in VFib arrest, defibrillated x1 followed by PEA arrest alternating with asystolic arrest during transport. Upon closer inspection, the defibrillator's monitor had assigned a spike for every large T wave as well as every QRS complex.
Soon afterward, the patient’s symptoms return along with lightheadedness, bradycardia, and hypotension. The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. The Queen of Hearts agrees: Around this time his initial high sensitivity troponin I resulted at 231 ng/L.
After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation. Of note — the QT interval of beat #5 ( blue line ) is markedly prolonged compared to the QT interval in the beginning of the tracing ( red line ). What does this ECG tell you?
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. Along with it, a guideline-based algorithm helps identify implantable cardioverter defibrillators.
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° A 12-lead ECG was recorded: There is sinus rhythm with RBBB and right axis deviation.
Despite immediate chest compressions, and multiple rounds of defibrillation, he could not be resuscitated. As crews were assessing the ECG he further elucidated that his pain was provoked during exertion with posterior radiation towards the intrascapular region, and associated with activity-limiting dyspnea.
She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). For example — bradycardia and AV conduction disturbances are not uncommon with Hyperkalemia , with these conduction disturbances most often resolving once serum K+ is corrected. The biopsy was consistent with cardiac sarcoidosis.
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. The corrected QT interval is extremely long, about 500 ms.
She was never defibrillated. As was seen in this case — defibrillation and/or overdrive pacing may be needed. She was given 3 mg IV epinephrine and multiple rounds of ACLS over approximately 20 minutes. Her husband stated that she had not been feeling well in the past 2 weeks and c/o dizziness as well as diarrhea. What do you think?
Cardioversion/defibrillation. Bradycardia. A partial list includes the following: Certain drugs ( antiarrhythmics; calcium channel blockers; ß-blockers; antianginals; psychotropic medications; alcohol; cocaine; other drugs ). Acute febrile illness. Variations in autonomic tone. Hypothermia. Ischemia/infarction.
Triage physician interpretation: -sinus bradycardia -lateral ST depressions While there are lateral ST depressions (V5, V6) the deepest ST depressions are in V4. When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. Triage EKG: What do you think?
The designation Brugada “ P henocopy” is given when an otherwise healthy patient has none of the factors associated with Brugada Syndrome — but only develops a Brugada-1 ECG pattern as a result of one of the above conditions — and, resolves this Brugada-1 pattern once the precipitating condition has been corrected.
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion.
Subcutaneous implantable cardioverter defibrillator was an innovation meant to reduce the lead related problems of conventional transvenous ICDs. But subcutaneous ICD cannot provide bradycardia and antitachycardia pacing as a transvenous ICD. A Modular Communicative Leadless Pacing-Defibrillator System. N Engl J Med.
Regardless of further evaluation, she should avoid bradycardia, AV nodal blockers, Na channel blockers, and fevers. --If Implantable Cardioverter-Defibrillator ), with long-term potential for device-related complications from the ICD, including inappropriate shocks?
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times.
ABSTRACT Introduction The subcutaneous implantable cardioverter defibrillator (S-ICD) is an alternative to a transvenous ICD in patients who meet the criteria for ICD implantation without concurrent need for cardiac pacing. The objective of this study is to examine the rates of and indications for S-ICD removal and extraction.
Although we lack details of events that followed Dr. Smith makes the key point that had this arrest witnessed by the medic team been the result of an acute cardiac event ( therefore, presumably VT or VFib ) prompt defibrillation by on-the-scene medics would most probably have resuscitated her.
There are 2 main options: Overdrive pacing could be considered and in the right clinical situation, this is often effective for reducing ventricular arrhythmias ( especially in the case of preventing pause induced or bradycardia-induced arrhythmias in association with QTc prolongation ). Try a different kind of antiarrhythmic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content