This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Circulation, Volume 150, Issue Suppl_1 , Page A4145609-A4145609, November 12, 2024. Electrocardiogram (ECG) and telemetry revealed junctional bradycardia with heart rate in 30s and sinus pauses (5-7 seconds). He was admitted for further workup of bradycardia. Patient did not report any symptoms and was hemodynamically stable.
There is sinus bradycardia with one PVC. Also notice that the arterial line mean arterial pressure is 63 mmHg, but there is no waveform (and SpO2 says "no pulse"), as the flow is continuous on ECMO and the LV function at this point was extremely poor, unable to add a pulse pressure. She then had a 12-lead: What do you think?
Abnormal readings can signal issues with circulation or lung function, prompting further investigation. Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical. Sleep Monitoring Quality sleep is essential for heart health.
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. = Would you approve her for a nonemergent surgical procedure?
Circulation: Cardiovascular Imaging. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). 2015, March 1). Cramer, M.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Serious AEs were rare; 1 patient in the etripamil arm experienced transient severe bradycardia and syncope, assessed as due to hyper-vagotonia.Conclusions:Intranasal etripamil 70 mg reduced VR and improved symptom-relief and treatment-satisfaction.
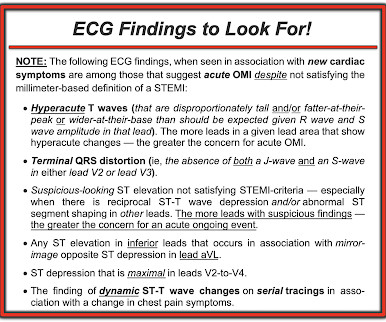
Dr. Smith circulated the initial ECG in today's case ( that I reproduce in Figure-1 ) to our group — initially without him yet knowing anything about this patient.
Athlete’s bradycardia due to increased parasympathetic tone and decreased sympathetic tone is a well-known observation. Though sinus bradycardia is usual, other abnormalities like sinus arrhythmia, sinus arrest, wandering atrial pacemaker and coronary sinus rhythm have been described. Circulation. Heart Lung Circ.
Use of drugs producing bradycardia like beta blockers in stages III and IV may precipitate low output state. Circulation. In stage IV, this restrictive filling pattern remains fixed even during Valsalva maneuver. Initial stages (I to III) are considered reversible with treatment. Stage IV is considered as advanced. 2012; 126: 138-141.
Whatever today's rhythm turns out to be — the "good news" is that the bradycardia and degree of AV block is likely to improve as soon as there is reperfusion of the "culprit" artery ( Therefore need for prompt cath with PCI ).
Triage physician interpretation: -sinus bradycardia -lateral ST depressions While there are lateral ST depressions (V5, V6) the deepest ST depressions are in V4. In this case, the vessel supplied a portion of the posterior LV circulation. The screening physician ordered an EKG and noted his ashen appearance and moderate distress.
This is sinus bradycardia. Thus, in ECG #1 — the Tall R in lead V1 + the more-peaked-than-expected chest lead T waves + all of those lateral lead Q waves were probably all findings reflective of this patient’s prior coronary injury and coronary anatomy ( with disease in the posterior and circumflex circulation ). The QRS is narrow.
Baseline bradycardia in endurance athletes limits the use of ß-blockers. Ballatore et al — Medicina (Kaunas) 55(8): 497, 2019 — and — Page et al — Circulation 107:1141-1145, 2003 ). Clinically — The importance of factoring in increased vagal tone as a contributing factor to AFib episodes — extends into management.
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Circulation 2014 7. -- McLaren JTT, Meyers HP, Smith SW, Chartier LB. This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chest pain.
After 13 minutes of ALS resuscitation, pulses were palpated indicating a return of spontaneous circulation. Crew notifies the received ED of an incoming post-arrest patient and notes a sinus bradycardia on their monitor, as seen in Figure 2. Figure 2 : This rhythm shows a sinus bradycardia at a rate between 30 and 40bpm.
There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
Our collaboration with Orchestra BioMed will explore how cardiac pacing can go beyond management of bradycardia and conduction disease to treat hypertension as well,” said Robert C. Circulation. Kowal, M.D., vice president and general manager of Cardiac Pacing Therapies within the Medtronic Cardiac Rhythm Management operating unit.
lidocaine) can result in severe bradycardia or asystole (Weinberg, Sedowski and Alexander, below) The presence of accelerated idioventricular rhythm does not affect prognosis, and there is no definitive evidence that, if left untreated, the incidence of VF or death is increased. Circulation Research , 56 (2), 184–194. Moffat, M.
Circulation, Volume 150, Issue Suppl_1 , Page A4140337-A4140337, November 12, 2024. Background:Cardiac output reserve and exercise capacity are strong predictors of life expectancy. Chronotropic incompetence (CI) is the inability to reach an age appropriate maximum heart rate with exercise.
The rule of thumb is less accurate, and the risk is higher because a long QT in the presence of bradycardia ("pause dependent" Torsades) predisposes to Torsades. 6) Use a different rule of thumb for bradycardia : Manually approximate both the QT and the RR interval. 3) At heart rates below 60, far more caution is due.
Circulation, Volume 150, Issue Suppl_1 , Page A4134483-A4134483, November 12, 2024. Introduction:European, American and UK guidelines all endorse the prescription of the 'four pillars' of treatment (ACE/ARBs, b-blockers, MRAs and SGLT2 inhibitors) for heart failure with reduced LV systolic function (HFrEF).
Circulation: Cardiovascular Quality and Outcomes, Ahead of Print. Acute kidney injury was the most frequent possible treatment complication (515 000 per year), and bradycardia had the highest mean hospitalization costs ($17 400 [95% CI, $17 200–$17 500]).CONCLUSIONS:The
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. mEq of K pushed fast and circulated theoretically would raise serum K immediately by 1.0
The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. The QRS complex in ECG #1 is wide.
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
A repeat ECG was performed as adult cardiology was asked to evaluate the patient for emerget PCI: Sinus bradycardia with persistent elevation in the inferior leads with reciprocal depression in aVL Patient was taken to cath lab with adult cardiology which revealed normal coronary arteries without evidence of occlusion MI. Circulation.
Perhaps because the bradycardia in vasovagal syncope is only one part of the autonomic response. Phase 4 block is also referred to as "bradycardia dependent block." Circulation , 143 (10), 10621065. A stunning result. One of many examples in medical history that remind us of the importance of blinding in clinical trials.
There are 2 main options: Overdrive pacing could be considered and in the right clinical situation, this is often effective for reducing ventricular arrhythmias ( especially in the case of preventing pause induced or bradycardia-induced arrhythmias in association with QTc prolongation ). Try a different kind of antiarrhythmic.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. Circulation Research , 114 (12), 18521866. Circulation , 92 (3), 657671. Circulation , 125 (3), 491496. Circulation , 145 (13), 10021019. link] Bentzon, J.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content