This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
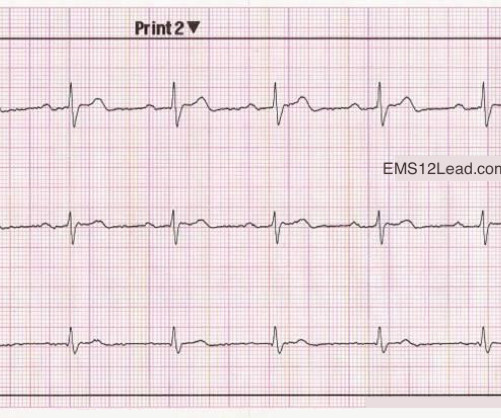
The chestpain quickly subsided. During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? He was intubated for altered mental status.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. If a patient presents with chestpain and a normal heart rate, or with shockable cardiac arrest, then ischemic appearing ST elevation is STEMI until proven otherwise.
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 1 remained in the hospital overnight. It was stented.
We have borderline sinus bradycardia with 1 ° AVB and occasional PACs. If this was a tachycardia at a rate of 150, it might appear to be a narrow complex tachycardia, when in fact, it would be a wide complex tachycardia! ECG diagnosis: Borderline sinus bradycardia, 1st degree AVB, RBBB, and occasional PACs.
Palpitations in a Young Healthy Male A pathognomonic ECG you should recognize instantly A middle-aged man with severe syncope, diffuse weakness Chestpain and Diffuse ST depression, with STE in aVR. You probably think it is left main. Are These Wellens' Waves?? Often more than one entity is operative as is likely in this case.
U waves may also be found in patients with LVH and/or bradycardia , or occasionally as a normal variant. This is often quite challenging to recognize — but the finding of negative U waves in a patient with chestpain is highly suggestive of ischemia ! N OTE # 2 — On rare occasions, the U wave may be negative. second ).
A recent similar case: A 40-something with chestpain. A useful classification of WCT ( W ide- C omplex T achycardia ) rhythms — separates them into those that are mono morphic ( with similar QRS morphology during the tachycardia ) vs those that are poly morphic ( in which QRS morphology varies ). Is this inferior MI?
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
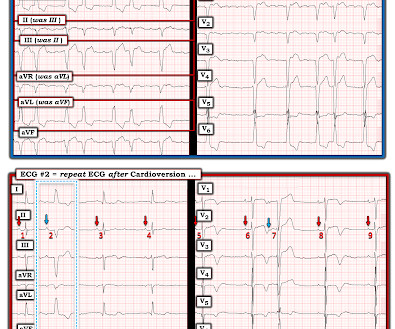
There was concern that the rhythm might represent ventricular tachycardia, so lidocaine was given and one attempt at cardioversion was performed. See our other countless hyperkalemia cases below: General hyperkalemia cases: A 50s year old man with lightheadedness and bradycardia Patient with Dyspnea. A Very Wide Complex Tachycardia.
There was no chestpain. Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. For example — bradycardia and AV conduction disturbances are not uncommon with Hyperkalemia , with these conduction disturbances most often resolving once serum K+ is corrected.
He did not have chestpain. ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Chestpain in high risk patient. Here is his triage ECG: What do you think? Is it STEMI?
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
All of the patients presented with chestpain , and they are all in triage. I completely agree with Dr. Nossen that in this patient with new CP and sinus tachycardia with LAHB — that the T waves in each of the inferior leads are hyperacute ( ie, clearly disproportionately "bulky" given size of the QRS in these leads ).
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms.
The rule of thumb is less accurate, and the risk is higher because a long QT in the presence of bradycardia ("pause dependent" Torsades) predisposes to Torsades. 6) Use a different rule of thumb for bradycardia : Manually approximate both the QT and the RR interval. 3) At heart rates below 60, far more caution is due. which is 0.6
A late middle-aged man presented with one hour of chestpain. There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. He complained of generalized weakness and left lower extremity numbness. What is it? Activate the Cath Lab?
Apparently he denied chestpain. Other than tachycardia, Other than slight tachycardia, vitals were within normal limits (including oxygen saturation). JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain. Here is his first ED ECG: What do you see?
Prior ECG on file: Sinus tachycardia, imperfect baseline, otherwise unremarkable. Triage ECG, with patient awake and complaining of right lower extremity pain: What do you see? Given the absence of chestpain — cardiac contusion is also unlikely. Acute coronary syndrome is unlikely to be one of those entities.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. It was from a patient with chestpain: Note the obvious Brugada pattern. A rectal temperature was obtained which read 107.9 This patient ruled out for MI.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Most physicians will automatically be worried about these symptoms. Frequent or repetitive PACs ii.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
In view of the clinical history ( ie, that this patient had a history of longstanding AFlutter but as far as we know, no chestpain ) this ST-T wave change most likely reflects a "memory" effect , in which there will often be ST-T wave abnormalities that persist for hours ( up to a few days ) following a long period of a sustained tachycardia.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. He told the patient this horrible news.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content