This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. Is there STEMI? Fortunately the patient was then taken for angiography.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0.
See our other countless hyperkalemia cases below: General hyperkalemia cases: A 50s year old man with lightheadedness and bradycardia Patient with Dyspnea. A woman with near-syncope, bradycardia, and hypotension What happens if you do not recognize this ECG instantly? Also: How did this happen? Is this just right bundle branch block?
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. Here is his triage ECG which was obtained at 20:34 during active pain.
A 50-something man presented in shock with severe chestpain. Here is his ED ECG: There is bradycardia with a junctional escape. There is an obvious inferior posterior STEMI(+) OMI. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. He appeared gray in color, with cool skin.
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive.
The patient presented with chestpain. If it is STEMI, it would have to be RBBB with STEMI. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Bradycardia. This ECG was sent from South Asia.
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ).
This was sent to me by a former resident from a community hospital: A middle-aged woman complained of chestpain and was seen in triage. The computer interpreted the ECG (GE Marquette 12 SL) as: "Sinus Bradycardia. Here it is: Computer interpretation: "Sinus bradycardia. She had a ECG recorded. Normal ECG."
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. What do you think?
The patient has acute chestpain. Any objective, rule-based analysis of this ECG would scream "STEMI" or "OMI". And I recognized this as a STEMI mimic. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. This was texted to me in real time.
The patient with no prior cardiac history presented in the middle of the night with acute chestpain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. Their apparently excessive length (QT interval) is due to bradycardia. This is a case I had quite a while back.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He wrote most of it and I (Smith) edited.
His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. The pain was completely resolved after coronary intervention. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. Blood pressure: 130/80 mmHg, heart rate: 45/min, respiratory rate: 18/min, SaO2: %98, body temperature: normal.
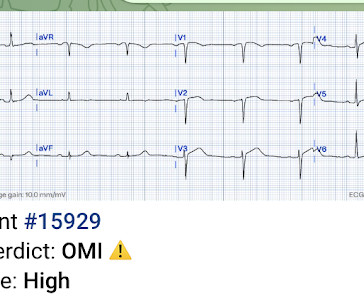
Written by Pendell Meyers A woman in her 50s presented with acute chestpain and lightheadedness since the past several hours. It does not meet STEMI criteria. Luckily, 45 minutes later, with ongoing pain and a troponin I that resulted at 136 ng/L, the ECG was repeated: What do you think now? Anyway, she does say OMI.
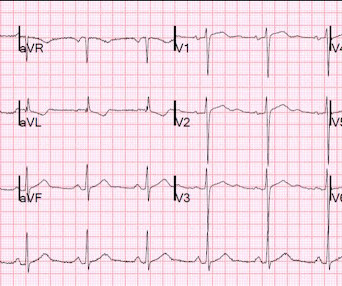
A middle-aged woman with a history of hypertension presented with typical chestpain. Here was her presenting ECG, with chestpain: Inferior leads show hyperacute T-waves and reciprocal STD in aVL, with a reciprocally hyperacute T-wave in aVL. Her BP was 160/80. This is all but diagnostic of inferior OMI.
A 40-something male with no previous cardiac disease presented with chestpain. The pain continued and the first high sensitivity troponin I returned at 105 ng/L Another ECG was recorded: The ST segment in aVF has flattened a bit, revealing that there is some STD in addition to the non-specific findings in III and aVL.
A late middle-aged man presented with one hour of chestpain. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. There is atrial fibrillation.
Apparently he denied chestpain. The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain. Canto et al.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion.
He did not have chestpain. Is it STEMI? Chestpain in high risk patient. Syncope and Bradycardia Syncope in a 20-something woman Long QT: Do not trust the computerized QT interval when the QT is long An Alcoholic Patient with Syncope Cardiac Arrest. Here is his triage ECG: What do you think?
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chestpain: V5 and V6 sure look like a STEMI For this ECG and chestpain in the ED, the Cath lab activated. There was no OMI.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Step 1 to missing posterior MI is relying on the STEMI criteria.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5
A 55 year old with no previous cardiac history presented with 3 hours of chestpain. The pain was persistent and reportedly still present at the time of the ECG. But if the pain is persistent, as reported, then the patient must go to the cath lab even if the ECG suggests reperfusion.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. What is it?
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The ECG shows sinus bradycardia but is otherwise normal. The patient said his chestpain was 4/10, down from 8/10 on presentation. The following ECG was obtained.
Now chestpain free. Repeat ECG showing no STEMI, only non-specific ST-segment and T-wave abnormalities, unchanged from prior" Transferred to surgery for exploration but diagnostic studies were too indeterminate to be certain of intra-abdominal pathology. There is a junctional bradycardia. She was taken to the cath lab.
We have borderline sinus bradycardia with 1 ° AVB and occasional PACs. ECG diagnosis: Borderline sinus bradycardia, 1st degree AVB, RBBB, and occasional PACs. Generally speaking, right bundle branch block does not mimic, or obscure, the ECG diagnosis of acute STEMI the way left bundle branch block does. What’s the rhythm?
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI.
The combination of absence of chestpain and history of LV aneurysm made it easy to assess that this patient does not have acute OMI. At this point — I learned a bit more about today's patient: The patient is a man who had an inferior STEMI in 2010. We know today's patient had a documented inferior STEMI in 2010.
Here is his previous ECG: This was my interpretation of the first ECG: Sinus bradycardia with less than 1mm ST elevation in V4-V6, elevated compared to the previous ECG, suggestive of lateral MI. Moreover, T-wave inversion in aVL was also found to be 100% sensitive and 86% specific for inferior STEMI. mm ST depression in aVL.
Here are inferior leads, and aVL, magnified: A closer inspection of the inferior leads and aVL Sinus bradycardia. She went on to describe her chestpain as a "buffalo sitting on my chest" and a "weird" sensation in her jaw for 1 hour prior to arrival, associated with lightheadedness and diaphoresis. What do you think?
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI.
Palpitations in a Young Healthy Male A pathognomonic ECG you should recognize instantly A middle-aged man with severe syncope, diffuse weakness Chestpain and Diffuse ST depression, with STE in aVR. You probably think it is left main. Are These Wellens' Waves??
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. It was from a patient with chestpain: Note the obvious Brugada pattern. Bicarb 20, Lactate 4.2,
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. There’s sinus bradycardia, normal conduction, normal axis, delayed R wave progression, and normal voltages. STEMI negative : the EMS automated interpretation read, “STEMI negative. Sinus bradycardia.”
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chestpain that feels like heartburn but that radiates to the left arm. There’s sinus bradycardia, first degree AV block, normal axis, delayed R wave progression, and normal voltages. Below is the ECG. Take home 1.
Note: according to the STEMI paradigm these ECGs are easy, but in reality they are difficult. Theres inferior STE which meets STEMI criteria, but this is in the context of tall R waves (18mm) and relatively small T waves, and the STD/TWI in aVL is concordant to the negative QRS. This was false positive STEMI with an ECG mimicking OMI.
Regardless of further evaluation, she should avoid bradycardia, AV nodal blockers, Na channel blockers, and fevers. --If The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. EP study to further risk stratify her is recommended, with ICD placement depending on the results.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content