This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity. The pain was located in the mid to left chest and developed after riding his bike.
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible.
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. The ECG does not show any definite signs of ischemia. The below ECG was recorded.
Written by Pendell Meyers A woman in her 50s presented with acute chestpain and lightheadedness since the past several hours. The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize.
The patient presented with chestpain. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. 2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
The patient’s chestpain spontaneously resolved before he was evaluated and has a repeat ECG obtained at 22:12 obtained shown below. Soon afterward, the patient’s symptoms return along with lightheadedness, bradycardia, and hypotension. It is unclear if he received aspirin at triage. This ECG is more difficult.
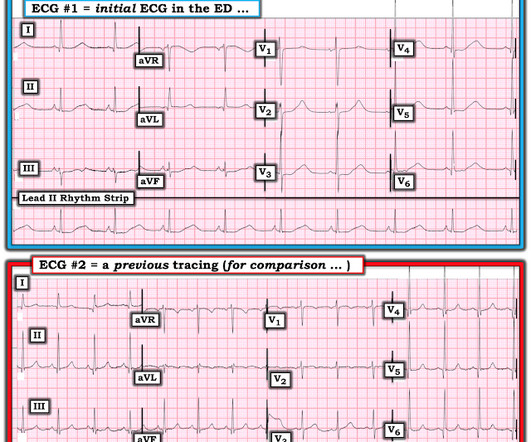
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. PEARL # 2: Applying PEARL #1 to today's case — the fact that this patient's symptoms began before ECG #1 was obtained, and that his chestpain had resolved by the time ECG #1 was recorded — strongly suggests that the "culprit" artery may have spontaneously opened.
He did not have chestpain. A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." Chestpain in high risk patient. Is it STEMI?
The patient with no prior cardiac history presented in the middle of the night with acute chestpain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. Their apparently excessive length (QT interval) is due to bradycardia. This is a case I had quite a while back.
The patient has acute chestpain. Here was my answer: "Not ischemia. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. This was texted to me in real time. What do you think? Maybe HOCM or another form of LVH. I would not activate cath lab.
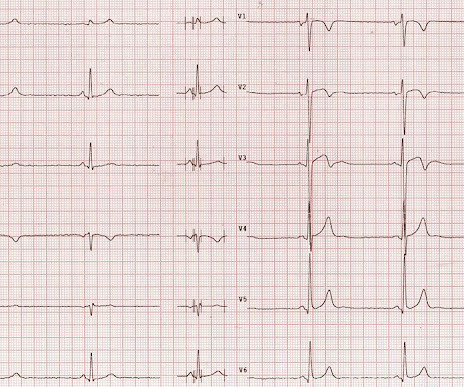
(This ECG could easily be seen in an ED chestpain patient, and I have seen many) What do you think? Description Sinus bradycardia. There is ST elevation in V2 and V3 There are inverted T-waves in V2 and V3 There are prominent U-waves in V2 and V3 Many responders were worried about ischemia or hypertrophic cardiomyopathy.
A 40-something woman with h/o obesity, hyperlipidemia, smoking, as well as cocaine and alcohol abuse presented with intermittent chestpain for 2-3 weeks that became constant in the last day. There is also some generalized weakness. There is some associated SOB, but no nausea and vomiting. Here is the initial EKG: What do you think?
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness.
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). QUESTIONS: HOW would you interpret the rhythm in Figure-1 ? Is this " high -grade" AV block?
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. There is no definite evidence of acute ischemia. (ie, The below ECG was recorded.
All of the patients presented with chestpain , and they are all in triage. Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. True Positive ECG#2 : Also sinus rhythm.
The chestpain quickly subsided. During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. Acute ischemia? Are you worried about OMI in this case? Use of QT-prolonging drugs?
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. The patient had none of these conditions.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? ST depression. Myocardial Contusion?
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The computer called "Sinus Bradycardia" only (implying that everything else is normal. The overreading Cardiologist called it only "Sinus Bradycardia" with no other findings. There is zero ST Elevation.
A 40-something male with no previous cardiac disease presented with chestpain. Here is his ECG: There is no clear evidence of OMI or ischemia. This is suspicious for inferior reciprocal At this point, with continued pain, cath lab activation is indicated. even in the absence of ECG findings.
This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5 100% LAD occlusion. He underwent CABG. QRS V2 = 15.5
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. The patient was still in pain, with a third troponin of 500.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. He complained of generalized weakness and left lower extremity numbness. What is it? Activate the Cath Lab?
If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms.
Here is his previous ECG: This was my interpretation of the first ECG: Sinus bradycardia with less than 1mm ST elevation in V4-V6, elevated compared to the previous ECG, suggestive of lateral MI. This is his first ECG in the department, which I saw as it was being printed: What do you think? Notice how useful serial ECGs are!
That said — obvious findings include: i ) Marked bradycardia! — This suggests ischemia of uncertain duration. MY " Q uick T houghts" on Today's CASE: The ECG in Figure-1 is highly concerning — so it is indeed fortunate that this elderly woman came to the ED when she did! be regular! —
Although in the context of chestpain such ST depression would be all but diagnostic of posterior OMI, one should make no conclusions in such an unusual case. In all leads, there is a 2nd wave after the initial QRS. This is an Osborn wave. I have not found any previous report of Osborn waves in RBBB.
Here are inferior leads, and aVL, magnified: A closer inspection of the inferior leads and aVL Sinus bradycardia. She went on to describe her chestpain as a "buffalo sitting on my chest" and a "weird" sensation in her jaw for 1 hour prior to arrival, associated with lightheadedness and diaphoresis. What do you think?
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. ST depression: is it ischemia? In my experience, Ive seen U waves not only with low K+/low Mg++ but also in patients with bradycardia, LVH, and sometimes in normal subjects.
Now chestpain free. There is a junctional bradycardia. Furthermore, there are T-wave changes in V2 and V3 which are highly suggestive of ischemia, but difficult to localize: anterior? ng/mL (not giving exact number, but significantly high) Now having frequent PVCs. Troponin was repeated and returned higher still.
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%.
If a patient presents with chestpain and a normal heart rate, or with shockable cardiac arrest, then ischemic appearing ST elevation is STEMI until proven otherwise. This, in turn, could produce platelet aggregation and vasospasm and result in an acute coronary syndrome." Clinical Context is everything !
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI.
There was no chestpain. Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). For example — bradycardia and AV conduction disturbances are not uncommon with Hyperkalemia , with these conduction disturbances most often resolving once serum K+ is corrected.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Lead V2 shows RR’ QRS configuration, and although ST depression is otherwise expected here, the discordance is a bit excessive.
U waves may also be found in patients with LVH and/or bradycardia , or occasionally as a normal variant. This is often quite challenging to recognize — but the finding of negative U waves in a patient with chestpain is highly suggestive of ischemia ! N OTE # 2 — On rare occasions, the U wave may be negative.
A recent similar case: A 40-something with chestpain. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? Is this inferior MI? Just as interesting is EKG 1, 24 minutes before the first: What do you think here?
A late middle-aged man presented with one hour of chestpain. There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content