This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
This was sent to me by a former resident from a community hospital: A middle-aged woman complained of chestpain and was seen in triage. The computer interpreted the ECG (GE Marquette 12 SL) as: "Sinus Bradycardia. Here it is: Computer interpretation: "Sinus bradycardia. She had a ECG recorded. Normal ECG."
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin.
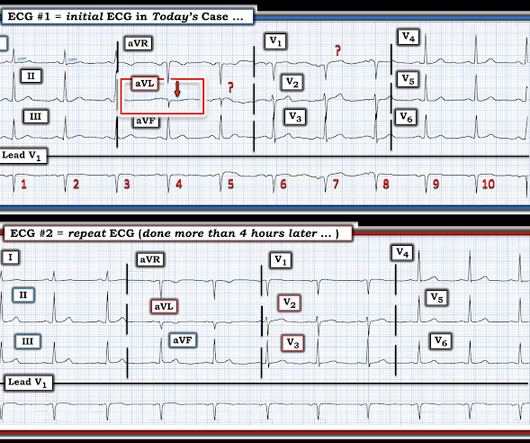
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. PEARL # 2: Applying PEARL #1 to today's case — the fact that this patient's symptoms began before ECG #1 was obtained, and that his chestpain had resolved by the time ECG #1 was recorded — strongly suggests that the "culprit" artery may have spontaneously opened.
He has now implemented the Queen of Hearts in his hospital. A 55 year old with no previous cardiac history presented with 3 hours of chestpain. The pain was persistent and reportedly still present at the time of the ECG. Jean-christophe Reiters, an interventionalist in Belgium. He has been following the blog for 4 years.
He did not have chestpain. The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Chestpain in high risk patient. Here is his triage ECG: What do you think? See these other relevant cases: What are these bizarre bigeminal PVCs?? Is it STEMI?
A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. The chestpain quickly subsided. She is healthy with no known cardiac disease. What do you think?
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The patient was extubated on Day-3 of the hospital stay. The below ECG was recorded.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 1 remained in the hospital overnight.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 Case 4 Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)?
Apparently he denied chestpain. JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain. We have countless cases of missed posterior MI on this blog, including these: Interventionalist at the Receiving Hospital: "No STEMI, no cath. Canto et al. Is that normal?
The relationship between low RHR and CI has yet to be described.Purpose:We hypothesize that resting sinus bradycardia (low RHR) could be a predictor of chronotropic incompetence and reduced exercise capacity.Methods:The derivation cohort consists of 201 patients with normal Bruce protocol treadmill stress echocardiogram. x age in years).Results:The
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. He complained of generalized weakness and left lower extremity numbness. What is it? Activate the Cath Lab?
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study. be regular! —
The rule of thumb is less accurate, and the risk is higher because a long QT in the presence of bradycardia ("pause dependent" Torsades) predisposes to Torsades. 6) Use a different rule of thumb for bradycardia : Manually approximate both the QT and the RR interval. 3) At heart rates below 60, far more caution is due.
Even if you don't see the OMI, you can usually prevent such a long delay to reperfusion by recording serial ECGs every 15 minutes for a patient with persistent chestpain. The rhythm in ECG #1 is sinus bradycardia and arrhythmia. Record serial ECGs every 15 minutes!! Hillinger et al.
Hospital transport was unremarkable. Smith and Myers found that in otherwise classic Wellens syndrome – that is, prior anginal chestpain that resolves with subsequent dynamic T wave inversions on the ECG – even the T waves of LBBB behave similarly. [2] He received a permanent pacemaker during the subsequent inpatient stay.
And she does not know that this is an overdose; she thinks it is a patient with chestpain!! This meets the Smith Modified Sgarbossa criteria, but the situation is wrong for diagnosing OMI!! By the way, the PM Cardio Bot Queen of Hearts says this is Not OMI with High Confidence. 3 hours later, this was recorded at a K of 2.8
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. See these similar cases: A man in his sixties with chestpain Why is there inferior ST elevation, and would you get posterior leads? Sudden CP and SOB with Inferior ST Elevation and in STE in V1.
A late middle-aged man presented with one hour of chestpain. There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. mg/dL [1.03 0.16
Written by Pendell Meyers We received a call from an outside hospital asking to transfer a "traumatic post arrest" patient. We were told that a young patient was brought in with altered mental status but complaining of right hip and/or leg pain after being found by his mother at the bottom of the stairs into the basement.
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. There’s sinus bradycardia, normal conduction, normal axis, delayed R wave progression, and normal voltages. Sinus bradycardia.” paramedic transportation to the ED as “chestpain, STEMI negative” 2.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Frequent or repetitive PACs ii.
Written by Kirsten Morrissey, MD with edits by Bracey, Grauer, Meyers, and Smith An older teen was transferred from an outside hospital with elevated serum troponin and and ECG demonstrating ST elevations. The workup at the transferring hospital yielded elevated troponin I at 18.1 He reported 1.5 mg/L and a normal WBC of 8.8.
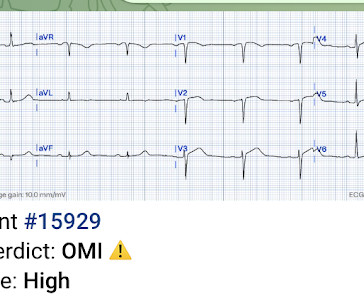
Despite the baseline artifact theres sinus bradycardia, convex ST elevation in III, reciprocal ST depression in aVL and possible anterior ST depression indicating inferoposterior OMI. He was given two separate sprays of nitroglycerin sublingually, neither of which improved his pain but did cause him to become briefly hypotensive ( 600 ng/L.
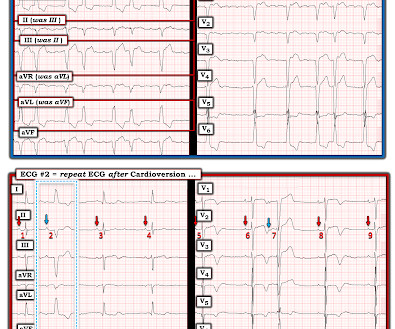
The patient tolerated cardioversion well and later that day was discharged from the hospital. ( PEARL # 2: Did you notice in the post-conversion tracing that there is ST segment coving with fairly deep T wave inversion in the chest leads? Serum electrolytes were normal at the time of cardioversion.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chestpain. En route to the next hospital, the paramedics recorded another 12-lead tracing. Also : See Ken Grauer's excellent comments at the bottom.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content